Chapter 14
Endocrine Investigations in Gynaecology
The term endocrine investigations is usually used
erroneously synonymous to hormonal blood tests. This concept should be changed. The term should be used instead to include all the available means to
examine and diagnose endocrine related problems. This is especially so as biochemical results are usually used to complement other diagnostic means, and
may be useless as stand alone indices. This chapter will promote this broader
concept and address history taking, clinical examination and imaging means, as
well as the biochemical tests used in this respect. There are many different
clinical scenarios when gynaecologists need to request specific hormonal tests
during investigations of certain cases. In other words, hormonal tests are
usually requested to verify or exclude a provisional diagnosis. These tests can
also be used to monitor patients response to treatment, or the progression of
the medical condition itself. There is an intricate interrelationship between
the normal physiology and pathophysiology related to the pituitary gland,
ovaries, adrenals and thyroid gland. Furthermore, many medications can affect
the function of these glands, and change their peripheral blood indices. An
important role for autoimmune disorders has already been addressed in the
previous chapters in this book, especially in relation to the adrenals and the
thyroid gland. Accordingly, gynaecologists must be able to appreciate, and
address the broader clinical problems, and request the right imaging and biochemical
hormonal and non-hormonal investigations. They should also be able to couple
these numerical results together, and in relation to the general clinical
picture.
Most endocrine investigations are conducted within a
gynaecological unit because of the following reasons:
- Abnormal
pubertal development, being delayed or precocious;
- Menstrual
dysfunction being polymenorrhoea, oligomenorrhoea,
amenorrhoea, or menorrhagia;
- Hyperandrogenisation
problems including acne, hirsutism, obesity and androgenic alopecia;
- Infertility
investigations including ovarian reserve, and monitoring ovulation
induction;
- Management
of abnormal pregnancies including ectopic or molar gestation;
- Perimenopausal
symptoms including premature ovarian failure.
Medical
history and physical examination
As for all medical problems, a thorough medical
history forms the platform for all endocrine investigations, depending on the
nature of the problem itself. The more usual questions should include the
pattern of onset of the problem being sudden or gradual, duration and
progression, any relevant related symptoms, history of excessive change in
weight, exercise level, medication or surgery, as well as the results of any
previous investigations. Symptoms suggestive of specific endocrinopathy should
also be explored, including hyperandrogenisation, fatigue, forgetfulness,
lethargy, fainting and dizzy spells, increased pigmentation, excessive hair
loss, polyurea and polydipsia. Childhood disease and developmental history are
important in relation to abnormal pubertal development, whether delayed or
precocious. History of malnutrition, chronic anaemia, tuberculosis and other
endemic diseases can give good clues to the origin of delayed puberty in
developing countries. Any significant family history, especially of maternal
age at the menopause should be elucidated. Another good example is history of
mental retardation in male siblings, especially in cases of premature ovarian
failure and fragile X syndrome.
General examination is important as well. The
patients general look, height, weight, and arms span are important parameters
to be ascertained. Blood pressure measurement is also important, as high levels
can be seen in patients with delayed puberty due to 17-hydroxylase deficiency,
and in patients with Cushings syndrome. Obesity and underweight conditions are
very important to ascertain with BMI calculations. It is difficult to give
specific scenarios about different physical outlooks, but the following
specific signs may indicate an endocrine dysfunction:
- Facial
plethora may be due to alcoholism or increased cortisol levels;
- Slow speech
and reactions, lack of concentration and forgetfulness may indicate severe
hypothyroidism;
- Exophthalmos,
warm damp palms, and hand tremors as signs of hyperthyroidism;
- Very tall or
short stature in relation to age, are important clues during
investigations of puberty related problems;
- Discrepancy
between height and arms span are important signs to verify; Upper to lower
body ratio is also important;
- Greasy or
dry skin can be secondary to hyperandrogenisation or hypothyroidism
respectively;
- Signs of
hyperandrogenisation including, acne, hirsutism and alopecia should be
recorded;
- Excessive
hair growth should be scored using the Ferriman and Gallwey scoring system
(1). A score > 8 is considered abnormal.
More information about this system and its limitations can be found in Chapter
6.
- Enlarged
thyroid gland can be a normal sign during puberty and pregnancy;
- Breast
development and staging using Tanners stages during investigations of
pubertal development problems;
- Sparse
development or absence of axillary and pubic hair in cases of autoimmune
adrenal insufficiency. This can also be seen in women with well developed
breasts, as seen in cases of androgen insensitivity (testicular
feminisation) syndrome;
- Acanthosis
nigricans at the back of the neck, in the axillae and under the breasts
have been associated with insulin resistance;
- The presence
of vitiligo, which indicates autoimmune dysfunction, is important when
dealing with such cases as premature ovarian failure;
- Low set
ears, webbing of the neck, bone deformities and other abnormal chromosomes
signs;
- Galactorrhoea may be present in about 50% of cases of
hyperprolactinaemia, but can be seen in women with normal prolactin
levels;
- Purple
striae ≥ 1.0 cm wide can indicate Cushings syndrome;
- Trunk
obesity and high waist / hip ratio as signs of androgenic obesity;
- Enlarged
clitoris as a sign of marked increase in androgens production as seen in
cases of virilization, together with deepening of the voice, body
masculinization and frontal hair recession;
- Neurological
signs especially in cases of precious puberty.
These are just examples of the physical signs seen in
patients presenting with problems which may have gynaecological endocrinology
background or origin. Gynaecological pelvic assessment should be performed,
when indicated.
Imaging
tests
Different imaging examinations are available,
depending on the condition being investigated. Transabdominal and transvaginal
ultrasound scan examinations are widely used to ascertain the presence and
normality of the internal genital organs. Testicles can be detected within the
inguinal canals in patients with testicular feminization syndrome. Diagnosis of
polycystic ovaries is a common objective, depending on the
patients presentation. The presences of 12 cysts in one or both ovaries, or an
ovarian size ≥10 cc are the two ultrasonic criteria adopted for the diagnosis
of polycystic ovaries (2). Diagnosis of
functional ovarian cysts, and endocrinologically active
solid ovarian masses can be helpful in certain cases. Adrenal masses can also
be detected ultrasonically, but are better diagnosed with MRI. Pituitary
adenomas are diagnosed with MRI which superseded the use of plain skull X-ray
and CT scanning, even as a first line imaging technique. Patients with high
prolactin levels are a prime target for this technique within the gynaecology
clinic. MRI of the brain is also indicated in cases with abnormal pubertal
development to exclude brain tumours, especially in the presence of
neurological symptoms or signs. The role of left hand and wrist X-ray in the
investigation and monitoring of abnormal pubertal development has already been
addressed in Chapter 2. Monitoring ovulation with transvaginal ultrasound scan
examination is important both for natural cycle tracking and during induction
of ovulation. A monitored natural cycle can also reveal the length of the
follicular and luteal phases, especially in patients with short cycles. Other
useful parameters include endometrial thickness and texture, and Doppler
assessment of uterine and endometrial blood flow. The superior role of
ultrasound scanning for monitoring induction of ovulation in comparison to
serial oestradiol estimations has already been discussed in Chapter 7.
Hormonal
tests
A thorough account has been given about biological
testing of oestrogens and progestogens effects and potency in Chapter 5. In a
clinical setup, the most practical similar bioassay test is the progestogen
challenge test, which is a diagnostic test for oestrogen exposure. The most
commonly used version of the test is to administer oral progestogens for 5-7
days, before being withdrawn. An oestrogen primed endometrium will bleed
following the withdrawal of the progestogen. This positive response is used to
indicate good oestrogen exposure, and to exclude hypoestrogenism. Negative
results can occur in well oestrogenised patients with endometrial adhesions, or
other causes of genital tract obstruction, and in cases of endometrial
tuberculosis. Accordingly, many authorities advised against the routine use of
the test, and recommended the use of blood hormone tests instead. Pregnancy is
a physiological cause for negative tests.
Following an appropriate clinical assessment, a
hormone test may be necessary to verify or refute a provisional diagnosis. It
is not uncommon for a hormonal test to be contradictory with a well reached
clinical impression. This may be due to different causes including:
1. Most hormones are
produced in pulses, and one test may not be a true representation of the
hormonal milieu. Examples of such difficulty can be seen with FSH, LH,
testosterone, oestradiol and insulin which are the more commonly requested
tests. The coefficients of variation (SD/Mean%) for a single estimation of
these hormones relative to multiple samples examined within 6 hours have been
reported as 14.7 % for FSH, 26.8 % for LH, 31.9 % for testosterone, 15.4 % for
oestradiol and 31.3 % for insulin by Abdel-Gadir et al in 1990 (3). In the same year,
serial screening with basal FSH estimations in different cycles has been
suggested by Scott et al (4), to compensate for the limited diagnostic and
predictive values of single FSH estimations.
- Hormones
have a circadian pattern. Few hormones have higher levels in the morning,
and timing the test for an afternoon slot will give an erroneous result.
Good examples are 17-hydroxyprogesterone which is used for the diagnosis
of 21-hydroxylase deficiency, androstenedione and testosterone. These
hormones are usually higher in morning blood samples following the adrenal
circadian rhythm. The circadian variations in cortisol levels are well
known.
- Hormone
levels vary during the different stages of the menstrual cycle and give
different results at different times. Early follicular phase assessment
reflects the basic gonadotrophins levels, before the expected rise during
the follicular phase and midcycle. High LH and testosterone blood levels
during the early follicular phase are usually associated with the polycystic
ovary syndrome, while higher levels of the same hormones during the
midcycle are normal physiological findings indicating ovulation. A further
example is FSH which needs to be tested on the 2nd or 3rd
days of the cycle, as the blood levels increase toward the middle of the
follicular phase. One further example is mid luteal phase serum
progesterone which needs to be tested about 7-9 days before the next
period. Accordingly, conducting the test arbitrarily on day 21 of a 35 day
cycle is not be useful, and gives a wrong diagnosis.
- Hormone
blood tests are affected by many drugs, and the patient should be asked
about such medication. This is especially so for hormonal treatment
including contraceptives, which can interfere with the endogenous
endocrine milieu. This is even valid for a progestogen challenge test
which may affect gonadotrophins blood levels, mainly LH. Induction of
ovulation with clomid can have a similar effect. It is a well known fact
that LH level is lower in cases of PCOS after induction of ovulation,
because of the modulatory effects of progesterone. Accordingly, such
hormonal treatment needs to be stopped for a month or two before
conducting meaningful hormonal tests. This statement is not valid for
patients on treatment for hyperprolactinaemia and hypo or hyperthyroidism,
when a hormonal test is performed to monitor response to treatment and
compliance.
- Certain
blood tests need to be performed after overnight fasting such as fasting
insulin and glucose levels, and the fasting lipid profile when
investigating women for insulin resistance.
- Serum
prolactin level can be affected even by the venepuncture used to collect
the blood sample itself. Furthermore, marginal elevations of TSH are not
uncommon, and usually settle with time. This can be a reflection of mild
transient thyroiditis, or even
laboratory errors due to cross reaction with other glycoproteins. In both
these scenarios the blood test needs to be repeated.
- Heterotypic
antibodies can affect immunoassays, and give
spurious results. Repeating the test using a different method will be
necessary.
- Marginally
elevated hormonal results are inconclusive, and should be repeated.
Examples of minor elevations of TSH and prolactin levels have already been
given. Dynamic tests may be necessary to reach a definitive diagnosis in
some cases. The mostly used test within a gynaecological setup is the
short synacthen test (Alliance Pharmaceuticals), which is used for confirmation
or exclusion of adrenal enzymatic deficiency. In this scenario
17-hydroxyprogesterone level is measured before and 60 minutes after a
bolus dose of synthetic ACTH (synacthen). An exaggerated response of
17-hydroxyprogesterone indicates adult onset 21-hydroxylase deficiency.
The result should be read according to the laboratory normal ranges, as
there are overlaps between normal responses and heterozygous enzymatic
deficiency. This test is also useful within a general endocrinology setup,
as a test for adrenal insufficiency. Different cortisol cut-off levels
have been used to indicate normal and abnormal responses after a synacthen
test (5). Studies using 1 µg synacthen
showed good reproducibility and higher sensitivity compared to the
standard test with 250 µg as reported by Abdu and Clayton in 2000 (6). The same authors reported that post synacthen
cortisol levels <400 nmol/L were diagnostic of adrenal insufficiency
and Levels >600 nmol/L practically excluded the condition. Conversely,
levels between 400 and 600 nmol/L were doubtful and should be interpreted
in the light of the clinical data. The appropriate timing for the post
synacthen blood test has also been investigated, and 60 minutes tests were
found to be essential to avoid false results retrieved after 30-minute
short synacthen tests (7).
Specific
clinical examples
1. Hormonal tests
for delayed and precocious pubertal development include FSH, LH, and
oestradiol. In these cases LH is more important than FSH to detect the
initiation of puberty, as the upper and lower levels of the pulse increase with
the progressive pubertal stages. In case of FSH, it is only the upper limit of
the range which increases during the initial stages of puberty. It is sometimes
difficult to ascertain whether normal pubertal development has started or not.
This is the case with isolated premature breast development (thelarche). In such cases there is
exaggerated FSH response to the GnRH challenge test. There is also a tendency
toward lower basal and post GnRH test LH levels than in other girls with
precocious puberty as shown by Della Manna et al in 2002 (8). In contrast, girls with
central precocious puberty had higher LH peak levels after GnRH injection,
compared to prepubertal girls as shown by the same authors. Nonetheless, this
dynamic test is not usually necessary, as baseline LH assessments are adequate
to make a diagnosis, and to monitor response after initiation of treatment.
This is especially so as Pescovitz et al in 1988 (9)
showed that girls with early central precocious puberty frequently had LH and
FSH responses to GnRH stimulation similar to the FSH predominant response of
girls with isolated thelarche. Measurement of testosterone and
17-hydroxyprogesterone blood levels is necessary in cases of precocious
heterosexual puberty. This is mainly to detect 21-hydoxylase deficiency, which
makes more than 90% of all cases of adrenal enzymatic deficiencies. In all cases
bone age assessment is an integral part of the work
scenario as discussed in Chapter 2. Furthermore, ultrasound scan examination
can show increased uterine and ovarian volumes, in addition to breast
enlargement in cases of normal or central precocious puberty (8).
2. The range of hormonal
investigations in patients with anovulatory menstrual dysfunction depends on
the presence of collateral symptoms. Basic investigations should include
gonadotrophins, oestradiol, thyroid stimulating hormone (TSH), free thyroxine
(T4) and prolactin estimations. In the presence of hyperandrogenic symptoms or
signs, adrenal and ovarian precursors and androgens should be investigated.
This should include morning blood tests for 17-hydroxyprogesterone,
androstenedione, testosterone and sex hormone binding globulin (SHBG). This
will allow calculation of the free androgen index (the level of testosterone
divided by SHBG). With mild elevation of 17-hydroxprogesterone level, a
synacthen test is necessary. With adult onset 21-hydroxylase deficiency, there
is an exaggerated increase in the level of 17-hydroxyprogesterone. The result
should be compared to the values set by the laboratory for normal, heterozygous
and homozygous response, as mentioned before. Basic morning
17-hydroxyprogesterone blood levels should also be used to monitor adequate
response to glucocorticoids replacement therapy in patients with 21 hydroxylase
deficiency. In all cases of suspected anovulation, transvaginal ultrasound scan
examination should be performed to ascertain the presence of polycystic
ovaries, as mentioned before.
3. The presence of
insulin resistance may be explored in cases of PCOS, especially
in obese women and those with history of gestational diabetes or family history
of type II diabetes mellitus. Fasting insulin level on its own is not a
satisfactory method to test for insulin resistance, because of the wide
variability in the results, and an isolated fasting glucose measurement is
utterly useless in this respect unless the patient is already diabetic. The
oral glucose tolerance test (OGTT) is generally recommended for that purpose.
However, for practical clinical purpose the fasting glucose /insulin ratio can
be used instead, as it had good predictive value of insulin response during
OGTT, and highly correlated with insulin sensitivity
(10, 11).
A fasting glucose (mg/dL) / insulin (µU/mL) ratio <4.5 had positive and
negative predictive values of 87% and 94% respectively for diagnosing insulin
resistance (11). So, it is more useful in
excluding the diagnosis than confirming it, which is still important
information for patients management. The homeostasis model assessment of
insulin resistance (HOMA-IR) is another method which also proved to be useful
in this respect (12). It correlated highly with
estimates obtained by using the euglycaemic and hyperglycaemic clamps and
fasting insulin concentration (13). A cutoff
level >2.5 was considered to be diagnostic of insulin resistance in adults.
HOMA-IR proved to be more reliable than fasting glucose/insulin ratio and
quantitative insulin sensitivity check index as shown by Keskin et al in 2005 (14). A higher cutoff point of 3.16 was considered to
be diagnostic for insulin resistance in adolescents by the same authors.
HOMA-IR can be calculated by multiplying fasting insulin level in µU/mL by
fasting glucose level in mmol/l, and divide the outcome by 22.5. The concept of
homeostasis model assessment is extended to include HOMA-B which measures
changes in pancreatic B-cell function. It is mostly used in research projects
and is calculated by the equation (20 x insulin level in µU/mL) / (glucose
level in mmol/L 3.5). High HOMA-IR and Low HOMA-B were found to be independently
associated with increased diabetic risk in a multiethnic cohort of women,
reflecting the value of HOMA indexes in epidemiologic studies (15).
4. Infertility
hormone investigations depend on the age of the patients, and their mode of
presentation. Patient with irregular menstruation should be investigated for
anovulation as discussed in section 2 above. Patients with regular periods need
only mid luteal serum progesterone assessment to document adequate ovulation.
The length of the cycle should be taken into consideration, as day 21
progesterone assessment will give wrong results in patients with regular cycles
longer than 28 days. The length of the follicular and luteal phases can be
accurately documented by ultrasound scan monitoring of the cycle. Women in
their mid or late 30s need to have their ovarian reserve assessed, irrespective
of their menstrual pattern. A recent study by Gleicher et al (16) investigated the aetiology of premature ovarian
aging, which is another name for reduced ovarian reserve. They reported that
16.2% of women had genetic, 38.8% autoimmune and 12.2% combined causes, whereas
33.8% were idiopathic with no identifiable cause. They concluded that premature
ovarian aging and premature ovarian failure should be considered as continuum,
and should be investigated accordingly. In a different context, it should be
appreciated that such testing is not only necessary during infertility
investigations, but is indicated also to screen women in their 30s who would
like to delay childbearing.
Assessment
of ovarian reserve
Follicle stimulating
hormone
Over the years great efforts have been made to assess
the number and quality of oocytes prior to assisted reproduction treatment
cycles. The emphasis has now moved to include assessment of infertile women
during basic hormonal investigations. Age as a single parameter is weak
predictor of ovarian reserve and response to controlled ovarian stimulation
with gonadotrophins (17). For many years, FSH
assessment on the 3rd day of the cycle was the only available
investigation to assess ovarian reserve. The value of high basal FSH level
during assisted reproductive treatment cycles has been reflected by a high
cancellation rate due to poor response. As a single indicator, it was shown to
have better predictive value than age alone in this respect (18). On the other hand, chronological age was
associated with lower implantation rates owing to poor oocyte quality (19, 20). Such reduced
embryos implantation capacity with age has been related to increased aneuploidy
rate (21). This pattern was
shown by other studies as well (22, 23). At the
same time, Levi et al in 2001 (24) related high
FSH levels to increased rate of pregnancy loss, regardless of the womans age.
They advised that patients should be counselled regarding the low probability
of conception, and low live birth rates. This view has not been supported by
other articles when young women with high FSH blood levels have been examined.
This was shown by a study published by van Rooij et al in 2003 (20) which examined young women with high FSH blood
levels, against women older than 40 years of age with normal FSH levels. The
young group with high FSH had more cycle cancellation than the older group with
normal FSH. Nevertheless, the young group with high FSH had better implantation
rate per embryo, and higher ongoing pregnancy rate per cycle and embryo
transfer, than the older age group with normal FSH levels. Poor responders in
both groups had lower pregnancy rate than good responders.
It is an established observation that normal FSH levels
are unreliable predictors of ovarian reserve. This can be a reflection of the
following points:
1. FSH is produced
in pulses, and timing of the blood sample may coincide with the peak or the
bottom of the pulse, giving different results. As discussed previously, the
coefficient of variation (SD/Mean%) for a single FSH reading relative to
multiple samples examined within 6 consecutive hours on the same day has been
reported as 14.7 % by Abdel-Gadir et al in 1990 (3).
2. There is
intercycle variability of basal FSH blood levels, being higher in few but not
all cycles. Normally cycling women over the age of 40 years who had a normal
day 3 FSH level have 50% chance of having an elevated day 3 FSH level in a
subsequent cycle (25).
3. FSH levels rise
late in comparison to inhibin B and antimullerian hormone, following the
decline in the number of follicles.
4. FSH level can be
negatively affected by the level of oestradiol in the same blood sample. A high
oestradiol level >200 pmol/l on the 3rd day of the cycle carries
similar bad prognosis as high FSH. This can be a reflection of rapid
recruitment, with a follicle reaching a larger size than usual on day 3 of the
cycle. This is usually seen in patients with polymenorrhoea and short follicular phases, as the follicle
has started growing earlier during the luteal phase of the previous cycle. This
is a reflection of the early rise in FSH level at that time of the previous
cycle. Alternatively, the high oestradiol level follows recruitment of multiple
intermediate size follicles by day 3 of the cycle; each producing its share of
oestradiol. Transvaginal scan examination will help in making a diagnosis, and
can differentiate between these two possibilities.
The following techniques have been used to improve
the predictive value of FSH:
· Repeat the test during successive cycles, which is time
wasting for patients who need to start fertility treatment;
· Take 3 samples within a short period of time on the same
day to cover for the pulse variability;
· The clomiphene citrate challenge test has been used as well. It entails FSH
estimation on the 3rd day of the cycle, followed by 100 mg clomid
every day from day 5 to 9 of the cycle. FSH level should be examined again on
day 10 of the cycle. A level >10 IU/L indicates a bad prognosis with reduced
ovarian reserve, as it is expected to be suppressed by the rising oestradiol
level. Higher cut-off levels of FSH have been suggested in the literature. The
test has no additional value in women who already showed high basal FSH levels.
Few studies have shown significant intercycle variability of the clomiphene
citrate challenge test results in the same patients (4,
26). Furthermore, the predictive or clinical value of the test was not
superior to that of a basal FSH level in combination with antral follicles
count (27).
· Both intranasal and subcutaneous GnRH stress tests have been used to check the ovarian reserve.
The injectable test entails measuring FSH blood levels before and one hour
after a bolus dose of subcutaneous or intravenous dose of GnRH. An exaggerated
increase in the level of FSH relative to the basal measurement indicates
reduced ovarian reserve. The intranasal test entails 6 hourly administration of
GnRH after measuring the basal levels of FSH and oestradiol. These same
hormones should be measured 24 hours later. Similarly exaggerated increase in
FSH level, and reduced oestradiol response are taken as markers of reduced
ovarian reserve. These tests are hardly used in clinical practice nowadays, and
will not be discussed any further.
It is evident that high early follicular phase FSH
blood levels are more reliable than normal levels in predicting the ovarian
reserve. Certain conditions should be excluded from this general statement. FSH
blood levels can be increased physiologically during puberty, after using oral
contraceptives and during lactation. Other conditions associated with elevated
FSH levels include excessive smoking, during recovery from hypothalamic
amenorrhoea, and after unilateral oophorectomy (28). Patients with hyperthyroidism can also have mild elevation of both FSH
and oestradiol, as discussed in Chapter 11.
High FSH may be caused by
direct ovarian problems related to several granulosa cells FSH receptors
polymorphisms, but 2 of them located at codon 307 and 680 are more frequent.
The amino acid asparagine (Asn) is replaced by serine (Ser) at position 680
(N680S), and threonine (Thr) is replaced by alanine (Ala) at position 307. The
two most common allelic combinations are Thr307/Asn680
and Ala307/Ser680 as reported by Théron-Gérard et al in
2007 (29). Patients are usually classified as
homozygous (Ser/Ser or Asn/Asn) or heterozygous (Asn/Ser). Homozygous patients
for the Ser680/Ser680 variant (N680S) have longer
follicular phase of the cycle and higher basal FSH blood levels (29, 30). The later
being a natural compensation to stimulate normal follicular growth despite
reduced FSH receptors sensitivity. These patients also need higher doses of
gonadotrophins and produce lower levels of oestradiol during induction of
ovulation, though they have normal number of follicles (31). Accordingly, Greb et al (31)
suggested more studies to investigate the role of routine genotyping for N680S
polymorphism to help with tailoring ovarian stimulation protocols to individual
patients needs.
Mothers of familial
dizygotic twins showed high basal FSH blood
levels and pulse frequency, not related to the normal age-induced reduction of
negative feedback mechanism, as reported by Lambalk
et al in 1998 (33). Hypothalamic and/or
pituitary neuroendocrine factors not related to GnRH were suggested as possible
causes. There was no change in FSH pulse amplitude or response to GnRH
stimulation, compared to control groups. At the same time, there were no
differences in basal or GnRH induced LH levels, oestradiol, inhibin A or
inhibin B levels between mothers of dizygotic twins and controls. Genetic
studies so far failed to pinpoint the exact mutations which may lead to
dizygotic twining. No linkage was found in correlation to mutations in the gene
coding transmembrane FSH receptors (FSHR) as reported by Montgomery et al in
2001 (34). Furthermore, rare mutations in growth
differentiation factor 9 (GDF9) may affect twining chances, but dizygotic
twining is not associated with common variations in GDF9 (35).
False high FSH results can
also follow the presence of heterotypic antibodies in a patients blood, which can
interfere with the immunoassay. Spurious high FSH level was reported in a 33
year old women who had regular cycles by Cahill et al in 1992 (36). She proved to
have normal levels when an alternative laboratory method was used. Such
antibodies are not species specific. They can be found in patients regularly
exposed to animals or their products. Blood transfusions and autoimmune
diseases, especially the rheumatoid factor, have also been mentioned as possible
causes.
Antral
follicles count
To overcome the limitations of FSH in predicting
ovarian reserve, many other parameters have been introduced as alternatives, or
to complement its role in this respect. Transvaginal ultrasound scan
examination is one such parameter. Ovarian size and antral follicles count
during the early follicular phase have been used.
Reduction
of ovarian size, irrespective of parity, after the age of 40 years has been
documented by Andolf et al in 1987 (37). As expected, a substantial decline in ovarian
size has also been noticed after the menopause (38).
These points were taken further by Lass et al in 1997 (39), who assessed ovarian response to induction of
ovulation with gonadotrophins in relation to ovarian volume. Women with ovaries
<3.0 cc in volume needed higher dosage of gonadotrophins, had higher
cancellation rate, and produced less follicles than women with larger ovaries.
Accordingly, the authors recommended that assessment of ovarian size to be an
integral part of the infertility evaluation. This concept was taken even
further by Tomás et al in the same year (40).
They found that patients with <5 antral follicle (2 - 5 mm in diameter) in
each ovary had lower response to gonadotrophins than patients with more antral
follicles. This parameter was found to be more sensitive than ovarian volume or
patients age alone. Accordingly, they recommended antral follicles count,
rather than ovarian volume, for counselling patients regarding their expected
response to induction of ovulation. Using the same parameter, Frattarelli
et al in 2003 (41) confirmed the high
cancellation (41%) and low pregnancy (23%) rates in women with £ 4 antral follicles. The more important finding was that no antral follicles count absolutely
predicted pregnancy or cycle cancellation. Nevertheless, a meta-analysis published
by Hendriks et al in 2005 (42) showed a superior predictive
value of antral follicles count over basal FSH toward poor response. These
points put together support the recommendation made earlier by Bancsi et
al in 2002 (43)
that antral follicles count should be used together with other endocrine
parameters for the assessment of ovarian reserve.
It is
evident that patients with small ovaries and those with low antral follicles
need higher gonadotrophins doses to secure a response, and to reduce the risk
of cycle cancellation, during assisted reproduction treatment cycles. This
should be taken into consideration especially with the increased cost involved.
A step-down induction protocol with initial high dosage may be a better
option to secure the initial recruitment of follicles before reducing the dose,
if that proved to be necessary.
Inhibin
B
Inhibin B is another product of the granulosa cells.
A substantial decline in its blood levels with no significant changes in
inhibin A or oestradiol has been reported in early
perimenopausal women with regular cycles (44, 45).
This was followed after a period of time, and changes in menstrual cyclicity,
by marked fall in inhibin A and oestradiol levels, and a rise in FSH level,
without any further changes in inhibin B. This is another sign that basal
FSH and oestradiol levels are not reliable markers of the early decline in
ovarian reserve. The value of inhibin B as a measure of ovarian reserve has
been shown by many studies. Women with blood levels less than 45 pg/ml on day 3
of the cycle had lower oestradiol levels after induction of ovulation, higher
cancellation rate and lower number of oocytes collected, in comparison to women
with higher blood levels (46). This finding was
contradicted by a study published by Corson et al in 1999 (47), who failed to
find any clinical value for testing inhibin B. This was not a common
observation, as many other articles confirmed its value in predicting ovarian
response to induction of ovulation. On the other hand, it has the same drawback
as basal FSH, because of the physiological variability during the different
stages of the same menstrual cycle. Accordingly, it must be assessed on days 2
or 3 of the cycle.
In a different approach, Kwee et al in 2004 (48) tested the
intercycle variability of basal inhibin B and oestradiol levels before and after
injecting 300 IU of recombinant FSH subcutaneously. There were no significant
differences in the increment of either hormone, when the test was performed
during different cycles. Because of the reproducibility of the results, they
considered this test to be more reliable than basal FSH assessment and the
clomiphene citrate challenge test. Both tests gave
significantly variable results when performed during different cycles.
Nevertheless, like all other invasive dynamic tests, it did not attract much
interest, and has not commanded popular use in routine clinical setups.
Antimullerian
hormone
Antimullerian hormone (AMH) is produced by the
granulosa cells in close proximity to the oocytes, and by few cells surrounding
the antrum of 4 6 mm antral follicles. These cells continue producing AMH
till further recruitment and development of the follicles into dominant ones or
their ultimate atresia. Human AMH is a dimeric glycoprotein with a molecular
weight of 140 kdaltons, and it is a member of the transforming growth factor
beta (TGF-b) family of growth and differentiation
factors (49). At the ovarian level, AMH is
involved with follicular steroidogensis, and regulation of ovarian activity. It
reduces granulosa cells aromatase activity and the number of LH receptors in
cultured granulosa cells, and regulates testosterone production by the theca
cells (50). Reduction of the aromatase enzymatic
activity affects the intraovarian androgen / oestrogen ratio, hence oocyte
function. A high ratio leads to follicular degeneration, whereas a low ratio
causes germinal vesicles rupture (51-53). On the other hand, AMH reduces follicular
sensitivity to FSH. Furthermore, oocytes upregulate AMH expression in granulosa
cells, depending on their developmental stage (54).
This led to the hypothesis that oocytes in growing follicles control primordial
follicles recruitment and development through the inhibitory effects of AMH.
AMH
level has a direct correlation with the number of antral follicles; hence it is
a good marker of ovarian reserve. It was more consistently correlated with the
degree of follicular depletion than inhibin B and antral follicles count, even in young
patients with high FSH levels (55). Furthermore, it has relatively stable serum
concentration within one year in premenopausal women, and can be measured with
good reproducibility using commercial kits (56). Additionally,
blood levels do not change during the menstrual cycles, and the test can be
performed at any time irrespective of the stage of the cycle. A meta-analysis
published by Broer et al in 2009 (57) showed that AMH is at least as accurate as the
antral follicle count in predicting poor response and non-pregnancy during IVF
treatment cycles. However, most of the present data stress the fact that AMH is
the best currently available test for ovarian reserve. Nevertheless, like all
other parameters it does not reflect the quality of the eggs, which is
controlled by the patient's age. Furthermore, it was not a better predictor of
pregnancy when compared to the other available tests (49).
It is interesting that a recent report showed that AMH levels were affected by
ethnicity. Its blood levels were found to be 25.2% and 24.6% lower in
Afro-Caribbean and Hispanic women respectively, when compared to White women,
after adjusting for age, body mass index and smoking (58).
This raises the need to establish different cut-off levels for different ethnic
groups, which allows better utilisation of the test results in modern day
cosmopolitan societies.
A
recent publication showed that AMH level was significantly reduced during oral
contraception use, with a trend toward lower levels during metformin therapy (59). The question here would be what is the recovery
time to normal levels once such mediation is stopped? This is necessary to know
if patients who come off the pill need to have their ovarian reserve
established. The same authors came to the conclusion that AMH is an accurate
marker of antral follicles pool in WHO-2 / PCOS women, but its measurement is
not likely to be helpful in the management of these patients (59). This may not be true when dealing with PCOS cases,
as patients with high AMH blood levels (≥ 7.7 ng/ml) are less likely to respond
to ovarian drilling (60). Accordingly, AMH can
be used together with LH to select PCOS patients who are more likely to respond
to this procedure.
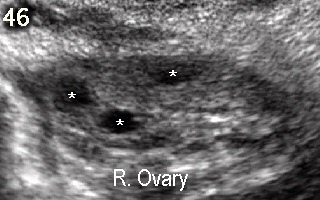
Figure 46 shows a small
right ovary with 3 antral follicles (2-5 mm in diameter) marked by asterisks on
day 3 of the cycle.
Figure 47 shows
a very small left ovary with no antral activity at all. These two pictures
belong to a 24 years old woman who had regular monthly cycles. Her day 3 FSH
level was 7.3 IU/L, but her AMH level was only 4.2 pmol/L. She needed 450 IU of
human menopausal gonadotrophin every day for 13 days to produce 3 follicles.
Three oocytes were collected and injected with her husbands sperm, during
intracytoplasmic sperm injection treatment cycle. Two oocytes were fertilized,
and were replaced on day 2 of the procedure. She conceived a single
intrauterine pregnancy and delivered a healthy baby at term. This case
reflected the unreliability of a normal day 3 FSH blood level in predicting the
ovarian response during an assisted reproduction treatment cycle. It also
showed the value of both transvaginal ultrasound scan examination and AMH in
this respect.
Figure 48 shows two small
ovaries with a single antral follicle in the left one. This 37-year old patient
had regular menstrual cycles with normal day 3 FSH blood levels (<10 IU/L).
Her AMH was only 1.73 pmol/L. She failed to respond to controlled ovarian
hyperstimulation with high doses of gonadotrophins injections. It was a further
example of how normal FSH blood levels failed to predict her ovarian response.
Other
clinical conditions
Human chorionic
gonadotrophin is another glycoprotein hormone which is used for the diagnosis
of normal and abnormal pregnancies, and as a tumour marker. The total molecule
cross-reacts with other glycoproteins due to the similarity of their a chains.
Accordingly, the ß subunit is used because of its specificity. The
three more common pathological conditions related to high human ßhCG blood
levels are ectopic pregnancies, gestational trophoblastic tumours, and ovarian
teratomas.
Ectopic pregnancies
With ectopic
pregnancies, a positive ßhCG test is associated with an empty uterus, and
occasionally a positive ultrasonic identification of an ectopic mass outside
the uterine cavity. Transvaginal ultrasound scan examination can give a very high
positive predictive value and helps with the diagnosis in 90% of the cases,
when performed by experienced personnel. An empty uterus with ßhCG level of
1500-2000 IU/ml indicates an ectopic pregnancy, as an intrauterine sac
should be seen at such levels. The most common ultrasound finding is the presence of a mass beside the
uterus on the same side as the corpus luteum, in almost 80% of the
cases. Viable ones with fetal heart activity are the least
common type. Depending on the stage at diagnosis,
variable amounts of fluid with floating particles can be seen in the pouch of
Douglas indicating intra-peritoneal leak of blood from the ectopic pregnancy. ßhCG blood levels are usually lower than those
expected for the period of amenorrhoea, and the rate of increase over a period
of time is also lower than expected for normal intrauterine pregnancies. The level of ßhCG
usually doubles, or at least increases by 1.66 fold every 2 3 days in 85% of
normal intrauterine pregnancies. In recent years, serum progesterone has been
used as an extra parameter for the diagnosis of ectopic pregnancies, as it has
a constant blood level during the whole of the first trimester. A blood level ≥
25 ng/ml is usually diagnostic of an intrauterine pregnancy. It excludes
an ectopic pregnancy with 97.4% certainty, in spontaneously conceived cycles.
Conversely, a level < 15 ng/ml has been reported in 81% of ectopic and 93% of
abnormal intrauterine pregnancies. It is also seen in 11% of normal
intrauterine pregnancies. It is evident that the higher the progesterone blood
level, the stronger its negative predictive value will be in excluding a
diagnosis of ectopic pregnancy. Accordingly, all three parameters (clinical,
scan examination and hormonal tests) should be combined to reach a diagnosis.
The use of hormonal tests in the follow up of cases managed conservatively, and
in the management of pregnancies of unknown location has reduced the need for
unnecessary surgery in many cases.
Gestational
trophoblastic tumours
Very high blood ßhCG levels are suggestive of
gestational trophoblastic tumours (GTT), which can be benign or cancerous. The
group includes molar pregnancy, persistent trophoblastic disease, placental
site trophoblastic tumours (PSTT), and choriocarcinomas. The intrauterine
contents can show a snowstorm appearance in cases of a complete mole, during
transvaginal ultrasound scan examination. Conversely, partial molar pregnancy
may look almost normal during ultrasound scanning. The ovaries are usually
enlarged with multiple corpora luteal cysts. Serial estimations of ßhCG levels
are used for monitoring response to treatment. Patients usually need other
investigation modalities including X-ray chest, CT scans, MRI, and even lumbar
puncture. A complete account about this subject is beyond the remit of this
chapter.
The use of ßhCG as a tumour marker is not limited
to trophoblastic diseases, as the level can also
be elevated in patients with other gynaecological neoplasms. Teratomas,
dysgerminomas and germinal cell tumours are such examples. In these cases, the
diagnosis is usually made with the help of ultrasound scan examinations or MRI.
Paradoxically, high ßhCG levels have been reported in patients with
vulvovaginal and cervical cancers. The prognosis was found to be worse for
patients with higher than normal ßhCG levels (61).
Other malignant and benign non gynaecological conditions were also associated
with high blood ßhCG levels. The list included melanomas, colonic, breast and
renal tact carcinomas (62-64). Despite the high ßhCG levels, trophoblastic cells
were not present in biopsies retrieved from these tumours. Benign conditions
associated with high ßhCG levels included liver cirrhosis, duodenal ulcer, and
inflammatory bowel disease. Accordingly, these conditions should be taken
into consideration when a high ßhCG level is detected in non pregnant women.
However, ßhCG is not a recognised method for the diagnosis or monitoring of any
of these conditions.
Many other hormones can also be used electively for
detecting pelvic tumours, or are chance findings in correlation to certain
gynaecological problems. AMH can be a biomarker of increased breast cancer risk (65), and
a marker of granulosa cell tumours which also produce very high levels of
oestradiol. This can cause long periods of amenorrhoea followed by excessive
breakthrough uterine bleeding. Such tumours also result in precocious isosexual
pubertal development. On the other hand, case reports of parasitic ovarian
leiomyomas presenting with endocrine related problems have been published.
Hyperandrogenic skin and hormonal changes have been reported in postmenopausal
women with ovarian leiomyoma due to theca cell reaction (66), and hilus cells hyperplasia (67). Similarly a case report of secondary amenorrhoea
caused by high inhibin B level secondary to a parasitic ovarian
leiomyoma has been published by Abdel-Gadir et al in 2010 (68). This patient resumed menstruating within one
month after excision of the ovarian fibroid.
Summary
This chapter has been written to complement the
information given in the previous chapters, with gynaecologists in mind. It is
meant to give a general overview of the different endocrine investigations used
in gynaecological practice. In many cases clinical history, physical
examination and imaging techniques provide the necessary information to reach a
diagnosis, with minimal need for elaborate hormone tests. Special efforts have
been made to emphasise the strength and limitations of the common hormone tests
used in gynaecological practice. The need for proper timing of blood samples
collection within the day, and in relation to the stage of the menstrual cycle
has been stressed. Any medication taken by the patient should be taken into
consideration when requesting a hormone test, and during the interpretation of
the results. Such tests should be used to complement the clinical impression,
and to extend the clinical judgement necessary for the management of any
particular case. Many results can be spurious for different reasons, and may
not agree with the general clinical picture. In such cases the examination
should be repeated for confirmation purpose, using a different method if
possible, before changing the patients management plan. Adequate knowledge of
the relevant basic Reproductive Endocrinology will allow better utilisation of
the available diagnostic means, facilitates proper patients care, and
eliminates misuse of resources.
References
1. Ferriman D and Gallwey JD. Clinical
assessment of body hair growth in women. J Clin Endocrinol 1961; 21: 1440-1447.
2. Revised 2003
consensus on diagnostic criteria and long-term health risks related to
polycystic ovary syndrome. Fertil Steril 2004; 81(1):19 25.
3. Abdel-Gadir A, Khatim MS, Mowafi RS, Alnaser HMI, Alzaid HN and Shaw RW.
Polycystic ovaries: do these represent a specific endocrinopathy? BJOG 1991;
98: 300 305.
4. Scott RT, Hofmann
GE, Oehninger S and Muasher SJ. Intercycle variability of day 3 follicle
stimulating hormone levels and its effect on stimulation quality in in-vitro
fertilization. Fertil Steril 1990; 54: 297 302.
5. Mansoor S, Islam N, Siddiqui I and Jabbar A. Sixty-minute post-synacthen
serum cortisol: a reliable and cost effective screening test for excluding
adrenal insufficiency compared to the conventional short synacthen test.
Singapore Med J 2007; 48(6): 519 523.
6. Abdu TAM and Clayton R. The low-dose synacthen test for the assessment
of secondary adrenal insufficiency. Curr Opin Endocrinol and Diabetes 2000;
7(3): 116 121.
7. Edavalath M, Hudson P and Leigh J. Comparison of 30 minute short
synacthen test and 60 minute short synacthen test for assessment of the
hypothalamo-pituitary adrenal axis. Endocrine Abstracts 2007; 13: 94.
8. Della Manna T, Setian N, Damiani D, Kuperman H, Dichtchekenian V.
Premature thelarche identification of clinical and laboratory data for the
diagnosis of precocious puberty. Rev Hosp Clin Fac Med Sao Paulo. 2002; 57: 49
- 54.
9. Pescovitz OH, Hench KD, Barnes KM, Loriaux DL, Cutler GB Jr. Premature
thelarche and central precocious puberty: the relationship between clinical
presentation and the gonadotropin response to luteinizing hormone-releasing
hormone. J Clin Endocrinol Metab. 1988; 67: 474 - 479.
10. Parra A, Ramirez A and Espinosa de los Monteros A.
Fasting glucose/insulin ratio. An index to differentiate normo from
hyperinsulinaemic women with polycystic ovary syndrome. Rev Invest Clin 1994;
46(5): 363 368.
11. Legro RS, Finegood D and Dunaif A. A fasting
glucose to insulin ratio is a useful measure of insulin sensitivity in women
with polycystic ovary syndrome. J Clin Endocrinol Metab 1998; 83: 2694 2698.
12. Katsuki A, Sumida
Y, Gabazza EC, Murashima S, Furuta M, Araki-Sasaki R, Hori Y, Yano Y and Adachi
Y. Homeostasis model assessment is a reliable indicator of insulin resistance
during follow-up of patients with type 2 diabetes. Diabetes Care 2001; 24(2):
362 3365.
13. Matthews DR,
Hosker JP, Naylor BA, Teacher DF and Turner RC. Homeostasis model assessment:
insulin resistance and B-cell function from fasting plasma glucose and insulin
concentrations in man. Diabetologia 1985; 28: 412 419.
14. Reskin M,
Kurtoglu S, Kendirci M, Atabek E and Yazici C. Homeostasis model assessment is
more reliable than the fasting glucose/insulin ratio and quantitative insulin
sensitivity check index for assessing insulin resistance among obese children
and adolescents. Pediatrics 2005; 115(4): e500 e503.
15. Song Y, Manson
JE, Tinker L, Howard B, Kuller LH, Nathan L, Rifai N and Liu S. Insulin
sensitivity and insulin resistance determined by homeostasis model assessment
(HOMA) and risks of diabetes in a multiethnic cohort of women: The womens
Health Initiative Observational Study. Diabetes Care 2007; 30(7): 1747 1752.
16. Gleicher N,
Weghofer A, Oktay K and Barad D. Do aetiologies of premature ovarian aging
(POA) mimic those of premature ovarian failure (POC)? Hum Reprod 2009; 24(10):
2395 2400.
17. Check JH, Lurie
D, Callan C, Baker, K and Benfer K. Comparison of the
cumulative probability of pregnancy after in vitro fertilization-embryo
transfer by infertility factor and age. Fertil Steril 1994; 61: 257 261.
18. Toner JP. The
significance of elevated FSH for reproductive function. Baillières Clin Obstet
Gynaecol 193; 7: 283 295.
19. van Kooij RJ,
Looman CW, Habbema JD, Dorland M, te Velde ER. Age-dependent decrease in embryo
implantation rate after in vitro fertilization. Fertil Steril 1996; 66: 769
775
20. van
Rooij IAJ, Bancsi LFJMM, Broekmans FJM, Looman CWN, Habbema DF and te Velde ER.
Women older than 40 years of age and those with
elevated follicle-stimulating hormone levels differ in poor response rate and
embryo quality in in-vitro fertilization. Fertil Steril 2003; 79
(3): 482 488.
21. Munne S, Alikani M, Tomkin G, Grifo J, Cohen J. Embryo morphology,
developmental rates, and maternal age are correlated with chromosome
abnormalities. Fertil Steril 1995; 64: 382 391.
22. Sharif K,
Elgendy M, Lashen H, Afnan M. Age and basal follicle stimulating hormone as
predictors of in vitro fertilisation outcome. Br J Obstet Gynaecol 1998; 105:
107 112.
23. Creus M, Penarrubia J, Fabregues F, Vidal E, Carmona F, Casamitjana R,
Vanrel JA and Balasch J. Day 3 serum inhibin B and FSH and age as predictors of
assisted reproduction treatment outcome. Hum Reprod 2000; 15: 2341 2346.
24. Levi A, Raynault
MF, Bergh PA, Drews MR, Miller BT and Scott Jr RT. Reproductive outcome in
patients with diminished ovarian reserve. Fertil Steril 2001; 76(4): 666 669.
25. Brown JR, Liu HC,
Sewitch KF, Rosenwaks Z and Berkeley S. Variability of day 3
follicle-stimulating hormone levels in eumenorrhoeic women. J Reprod Med 1995;
40: 620 624.
26. Hannoun a, Abu
Musa A, Awwad J, Kaspar H and Khalil A Clomiphene citrate challenge test: cycle
to cycle variability on cycle day 10 follicle stimulating hormone level. Clin
Exp Obstet Gynecol 1998; 25: 155 156.
27. Hendriks J,
Broekmans FJM, Bancsi LFJM, de Jong FH, Looman CWN and te Velde ER. Repeated
clomiphene citrate challenge testing in the prediction of outcome in IVF: a
comparison with basal markers for ovarian reserve. Hum Reprod 2005; 20(1): 163
169.
28. Lambalk CB and de Koning CH. Interpretation
of elevated FSH in the regular menstrual cycle. Maturitas. 1998;
30(2): 215 - 220.
29. Théron-Gérard L, Pasquier M, Czernichow C, Cédrin-Durnerin I and Hugues
J. Follicle-stimulating hormone receptor polymorphism and ovarian function.
Gynecol Obstet Fertil 2007; 35(2): 135 134.
30. De Koning CH,
Benjamins T, Harms P, Homburg R, Van Montfrans JM, Gromoll J, Simoni M and
Lambalk CB. The distribution of FSH receptor isoforms is related to basal FSH
levels in subfertile women with normal menstrual cycles. Hum Reprod. 2006; 21(2): 443 - 446.
31. Behre HM, Greb RR,
Mempel A, Sonntag B, Kiesel L, Kaltwasser P, Seliger E, Röpke F, Gromoll J,
Nieschlag E and Simoni M. Significance of single nucleotide polymorphism in
exon 10 of the follicle-stimulating hormone (FSH) receptor gene for the ovarian
response to FSH: a pharmacogenetic approach to controlled ovarian
hyperstimulation. Pharmacogenet Genomics 2005; 15(7): 451 456.
32. Greb RR, Behre HM, and
Simoni M. Pharmacogenetics in ovarian stimulation current concepts and future
options. Reprod Biomed Online 2005; 11(5): 589 600.
33. Lambalk CB, Boomsma DI, de Boer L, de Koning CH,
Schoute E, Popp-Snijders C and Schoemaker J. Increased levels and pulsatility of
follicle-stimulating hormone in mothers of hereditary dizygotic twins. J Clin
Endocrinol & Metab 1998, 83 (2): 481 486.
34. Montgomery GW, Duffy DL, Hall J, Kudo M,
Martin NG, and Hsueh AH. Mutations in the follicle stimulating hormone receptor
and familial dizygotic twinning. Lancet 2001; 357: 773 774.
35. Montgomery GW, Zhao ZZ, Marsh AJ, Mayne R, Treloar SA, James M, Martin
NG, Boomsma DI and Duffy DL. A deletion mutation in GDF9 in sisters with
spontaneous DZ twins. Twin Res 2004; 7(6): 548 555.
36. Cahill DJ, Fox R, Thomas PH. Spurious
elevation of follicle stimulating hormone. Acta Obstet Gynecol Scand 1992;
71(5): 388 389.
37. Andolf E,
Joregensen C, Svalenius E and Sunden B. Ultrasound measurement of the ovarian
volume. Acta Obstet Gynecol 1987; 66: 387 389.
38. Higgins RV,
van-Nagell JR, Donaldson ES, Gallion HH,
Pavlik EJ, Endicott B and Woods CH. Transvaginal
sonography as a screening method for ovarian cancer. Gynecol Oncol 1989; 34:
402 406.
39. Lass A, Skull J,
McVeigh F, Margara R and Winston RML. Measurement of ovarian volume by
transvaginal sonography before ovulation induction with human menopausal
gonadotrophin for in vitro fertilization can predict poor response. Hum Reprod
1997; 12(2): 294 297
40. Tomás C,
Nuojua-Huttunen S and Martikainen H. Pretreatment transvaginal ultrasound
examination predicts ovarian responsiveness to gonadotrophins in in-vitro
fertilization. Hum Reprod 1997; 12(2): 220 223.
41. Frattarelli
JL, Levi
AJ, Miller
BT and
Segars JH. A prospective assessment of the predictive
value of basal antral follicles in in vitro fertilization cycles. Fertil Steril
2003; 80: 350 355.
42. Hendriks DJ,
Ben-Willem Mol J, Bancsi LFJMM, te Velde ER and Broekmans FJM. Antral follicle
count in the prediction of poor ovarian response and pregnancy after in vitro
fertilization: a meta-analysis and comparison with basal follicle-stimulating
hormone level. Fertil Steril 2005; 83: 291 301.
43. Bancsi
LFJMM, Broekman
FJM, Marinus J. C. Eijkemans MJC, de Jong FH, Habbema DF, and te Velde ER. Predictors
of poor ovarian response in in-vitro fertilization: a prospective study
comparing basal markers of ovarian reserve. Fertil Steril 2002; 77(2): 328
336.
44. Burger
HG, Dudley EC, Hopper JL, Groome N, Guthrie JR, Green A, Dennerstein L. The
endocrinology of menopausal transition: a cross-sectional study of a
population-based sample. J Clin Endocrinol Metab 1995; 80: 3537 3545.
45. Burger HG, Cahir
N, Robertson DM, Groome NP, Dudley E, Green A and Dennerstein L. Serum inhibins
A and B fall differentially as FSH rises in perimenopausal women. Clin
Endocrinol (Oxf) 1998; 48(6): 809 813.
46. Seifer
DB, Lambert-Messerlian G, Hogan JW, Gardiner AC, Blazar AS, Berk CA. Day 3
serum inhibin B is predictive of assisted reproductive technologies outcome.
Fertil Steril 1997; 67: 110 114.
47. Corson SL,
Gutmann J, Batzer FR, Wallace H, Klein N and Soules Mr. Inhibin B as a test of
ovarian reserve for infertile women. Hum Reprod 1999; 14(11): 2818 2821.
48. Kwee J, Schats R, McDonnell JM, Lambalk
CB and Schoemaker J. Intercycle variability of ovarian reserve tests: results
of a prospective randomized study. Hum Reprod 2004; 19(3): 590 595.
49. Fiçicioğlu C,
Kutlu T, Baglam E. Bakacak Z. Early follicular antimullerian hormone as an
indicator of ovarian reserve. Fertil Steril 2006, 85(3): 592 596.
50. Cook CL, Siow Y,
Taylor S, Fallat ME. Serum mullerian inhibiting substance levels during normal
menstrual cycles. Fertil Steril 2000, 73: 859 861.
51. Filicori M,
Flamicnic R. The role of luteinizing hormone in folliculogenesis and ovulation
induction. Fertil Steril 1999; 71: 405 414.
52. Teixeria J, Maheswaran S, Donahoe TK.
Mullerian inhibiting substance: an instructive development hormone with
diagnostic and possible therapeutic applications. Endocrin Rev 2001; 22: 657
674.
53. Gruijters MJ, Visser JA, Durlinger AL,
Themmen AP. Anti-Mullerian hormone and its role in ovarian function. Mol Cell Endocrinol 2003; 211: 85 90.
54.Salmon NA, Handyside AH and Joyce IM.
Oocyte regulation of anti-mullerian hormone expression in granulosa cells
during ovarian follicle development in mice. Dev Biol 2004; 266: 201 208.
55. Knauff EAH, Eijkemans MJC, Lambalk CB, ten Kate-Booij
MJ, Hoek A, Beerendonk CCM, Laven JSE, Broekmans FJM, Themmen APN, de Jong and
Fauser BCJM. Anti-Mullerian hormone, inhibin B, and antral Follicle
count in young women with ovarian failure. J Clin Endocrinol & Metab 2008;
94 (3): 786 - 792
56. Dorgan JF, Spittle CS, Egleston BL, Shaw CM, Kahle LL and Brinon LA.
Assay reproducibility and within-person variation of mullerian inhibiting
substance. Fertil Steril; 94(1): 301 304.
57. Broer SL,
Ben Willem B,
Hendriks D, and Broekmans FJM. The role of antimullerian hormone in prediction of outcome after IVF:
comparison with the antral follicle count. Fertil Steril 2009; 91(3): 705
714.
58. Seifer DB,
Golub ET,
Lambert-Messerlian, Benning GL, Anastos K, Watts DH, Cohen MH, Karim R, Young MA, Minkoff H and Greenblatt RM. Variations in serum mullerian inhibiting substance between white, black,
and Hispanic women. Fertil Steril 2009; 1674 1678.
59. Fabregues F and Castelo-Branco J. The effect of different hormone
therapies on anti-mullerian hormone serum levels in anovulatory women of
reproductive age. Gyn Endocrinol 2011; 27(4): 216 224.
60. Amer
SA, Li TC and Ledger WL. The value of measuring antimullerian hormone in women
with anovulatory polycystic ovary syndrome undergoing laparoscopic ovarian
diathermy. Hum Reprod 2009; 24(11): 2760 2766.
61. Carter PG, Iles RK, Neven P, Ind TE, Shepherd JH, Chard T. Measurement of urinary beta core fragment of human chorionic gonadotrophin in women with vulvovaginal malignancy and its prognostic significance. Br J Cancer. 1995; 71(2): 350 - 353.
62. Doi F, Chi DD, Charuworn BB, Conrad AJ, Russell J, Morton DL, Hoon DS. Detection of beta-human chorionic gonadotrophin mRNA as a marker for cutaneous malignant melanoma. Int J Cancer. 1996; 65(4): 454 - 459.
63. Halim AB, Barakat M, el-Zayat AM, Daw M, el-Ahmady O. Urinary beta-HCG in benign and malignant urinary tract diseases. Dis Markers. 1995; 12(2): 109-115.
64. Ayala AR, Saad A, Vazquez X, Ramirez-Wiella G, Perches RD. Human chorionic gonadotropopin immunoreactivity in serum of patients with malignant neoplasm. Am J Reprod Immunol. 1983; 3(3): 149 151.
65. Dorgan JF, Stanczyk FZ, Egleston BL, Kahle LL, Shaw CM, Spittle CS,
Godwin AK and Brinton LA. Prospective case-control study of serum mullerian
inhibiting substance and breast cancer risk. J Natl Cancer Inst 2009; 101(21):
1501 1509.
66. Mallya S,
MacFarlane IA, Taylor W and Van Heyningen C. Thecal cell reaction associated
with an ovarian leiomyoma and presenting with virilization. Gynecol Endocrinol
1990; 4(14): 271-6.
67.Parish JM, Lufkin
EG, Lee RA and Gaffey TA. Ovarian leiomyoma with hilus cell hyperplasia that
caused virilization. Mayo Clin Proc 1984; 59(4): 275 - 277.
68. Abdel-Gadir A, Francis ND, Oyawoye OO and
Chander B. Secondary amenorrhoea with high inhibin B level caused by parasitic
ovarian leiomyoma. Gynecol Endocrinol 2010; 26(2): 93 95.