Chapter 6
Polycystic Ovary Syndrome
Polycystic ovary syndrome is the most common female endocrinopathy, and
could affect 3.5-11.2% of all women within their reproductive years (Knochenhour et al, 1998 (1). This wide variation in
reporting the real incidence might reflect the different diagnostic criteria
used. On the other hand ultrasonically diagnosed polycystic ovaries have been
reported in 16-25% of women with regular menstruation (Polson
2, Abdel-Gadir 3, and Wong 4). Variable familial expression in sisters
has been reported, and both autosomal dominant and sex linked transmission
modes have been described. However, most women with PCOS showed normal 46XX
chromosome, but some could also show dermatoglyphic male pattern. Though
unusual dermatoglyphic patterns relate to genetic disorders (Shiono 1986 5, Katznelsan 1982 6),
excessive intrauterine exposure to androgens was thought to be the cause in
patients with PCOS. A distinction between PCOS and the mere ultrasound
diagnosis of PCO is clinically necessary, but some evidence showed that such
distinction might not be as strict as previously suggested in many cases (Abdel-Gadir et al 1992 3, Carmine
and Lobo 1999 7 and Chang et al 2000 8).
Historic
considerations
Certain milestones exist in our current understanding of PCOS. The first
description of polycystic ovaries was recorded by Antonio Vallisneri in 1721. The
English translation of the Italian text was reported as follows: Young married
peasant women, moderately obese and infertile, with two larger than normal ovaries,
bumpy, shiny and whitish, just like pigeon eggs (Cindy
Farquhar et al 2000 9). This was followed by a description of sclerocystic
ovarian changes by Lisfranc in 1830. A similar pattern was then described respectively
by Chereau in 1844, Tilt in 1850 and Gallard in 1873, as reported by ODowd et al in 2000 (10).
However, the syndrome had its name and fame in modern medicine by 1935 when Stein and Leventhal (11)
described a combination of amenorrhoea, obesity and hirsutism in women with
enlarged ovaries. Adhering to this combination of symptoms and signs before
making a diagnosis, would exclude many of the patients with the syndrome as we
know it now.
The endocrine revolution in the diagnosis of PCOS has been started by McArthur et al in 1958 (12),
when they first described high LH levels in the urine of patients with
polycystic ovaries. High androgens levels were first reported in patient with
polycystic ovaries by De Vane et al in 1975 (13). This was followed by the documentation
of normal luteinising hormone blood levels in women with PCOS by Rebar in 1976 (14). Ultrasound reporting of the
ovarian polycystic pattern was first described by Swanson
et al in 1981 (15), followed by Hann et al in 1984 (16), before been objectively quantified by Adams et al in 1985 (17). Finally the association of
PCOS with insulin resistance was described by Kahn et
al (1976, 18), and became a major issue in the aetiology and morbidity
of PCOS. Further discussion of all these parameters would be found in the
corresponding parts of this chapter.
Traditionally, an ovary was described as polycystic when it contains 10
or more small cystic areas less than 10 mm in diameter in one ultrasound plane
(Adams et al 1985) (17).
Most of the clinical, endocrine, biochemical and Doppler ultrasound research
was conducted in patients diagnosed on the basis of this criterion, plus the
other clinical and biochemical parameters of anovulation and hyperandrogenism.
A new consensus has been agreed by the Rotterdam Study
Group (19), that 12 or more cysts in the
whole ovary should be used as a new parameter for the ultrasonic diagnosis of
PCO. This new ultrasound criterion is less stringent than the previous one, and
many normal patients would be included in such a diagnosis.
Development
of polycystic ovaries
Normally, as many as 10-20 follicles are recruited each cycle, but most
of them arrest before reaching full maturation, because of the dominant effect
of the leading follicle. Through oestradiols negative feedback mechanism, FSH
production by the pituitary gland is reduced. The dominant follicle would
continue growing because it had already developed a good microvascular blood
flow, and enough FSH receptors, with adequate aromatase enzyme activity to
maintain an oestrogenic intrafollicular environment. Smaller follicles would stop
growing because of their dominant androgenic endocrine milieu. Many researchers
have documented 2-3 fold increased development of pre-antral and antral
follicles in polycystic compared to normal ovaries (Hughesdon
1982 (20), Maciel 2004 (21) and Webber 2003 (22). Most of these follicles would
stop growing because of the abnormal hormonal signalling and the high
androgenic environment within the ovaries (Jonard and
Dewailly 2004, (23). Accumulation of such small cysts (underdeveloped
follicles) leads to the characteristic polycystic appearance which is more
common under the age of 35 years than in older women (Abdel-Gadir
et al (24). These cystic areas form a wide spectrum of growing
follicles and atretic cysts. On one side there are many growing follicles and
few atretic cysts. On the other end of the spectrum, there are many atretic
cysts and few growing follicles. Most cases fall in between these two extremes.
This could explain the differences in response shown by patients with
polycystic ovaries during induction of ovulation. It is not possible to
differentiate between these patterns during basic ultrasonography. Women with
more follicles would be expected to respond more quickly than those with
atretic cysts. The final destiny of the atretic cysts theca cells would be an
addition to form extra secondary ovarian stoma.
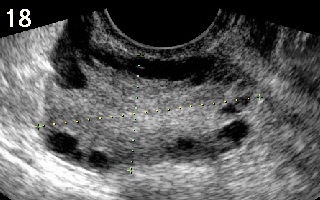
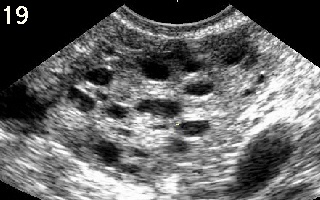
Better pictures became available since the advent of transvaginal scan
examination showing different patterns of cyst distribution within the ovaries:
- Cysts could be arranged under the
capsule giving the classical subcapsular pattern which is featured in
almost all articles and books.
- Cysts might be universally dispersed all
over the ovarian stroma.
- One ovary could
have a universal and the other subcapsular pattern of cysts
distribution.
- Few patients might have only one
polycystic ovary.
- Cysts could be localised to only one
part of an ovary.
A view was held previously that cysts distribution within the polycystic
ovaries could be a reflection of different endocrine patterns (Yen SS, 1980 (25). This was not the case as Abdel-Gadir et al in 1991 (26)
showed that basic and pulsatile patterns of FSH, LH and testosterone were not
related to the pattern of cysts distribution. This later view was upheld by the
recent consensus meeting on PCOS held in Rotterdam in
2003 (19), which also recommended that
increased stromal echogenicity should be excluded from the diagnostic criteria.
A volume ≥10 ml has been reaffirmed as a diagnostic criterion. Furthermore,
they suggested that one ovary showing a polycystic pattern in enough to make
the diagnosis in the presence of other diagnostic criteria. The significance of
volume has been shown in a previous study which documented better and quicker
response of patients with PCOS and larger ovaries to induction of ovulation with
gonadotrophins than others with smaller yet polycystic ovaries (Abdel-Gadir, (27). However, no difference could be
detected in the duration of symptoms, LH or testosterone blood levels or pulse
pattern between the two groups (Abdel-Gadir, (26).
This observation was in agreement with a previous statement made by Givens et al in 1976 (28) that normal size polycystic
ovaries might have similar histological and biochemical abnormalities as
enlarged ones. In this context volume could be more useful as a prognostic
parameter for better response to induction of ovulation with gonadotrophins,
rather than a reflection of the extent of derangement of the endocrine milieu,
or severity of the PCOS condition.
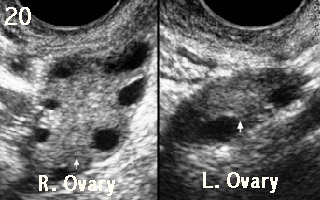
Figures 18 and 19 shown below demonstrates two ovaries with classical subcapsular and universe cyst distribution. Figure 20 on polycystic and one normal ovary. Note the difference in the size between the two ovaries (11.0 vs 2.7 cc) All three patients were hyperandrogenic and had irregular periods.
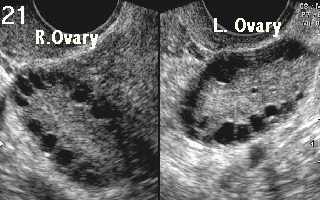
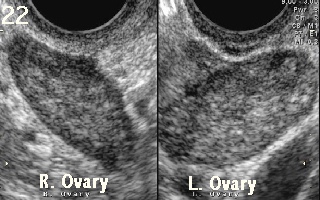
Prolong use of a combined oral contraceptive pill can affect ovarian morphology and volume, which can mask the polycystic pattern. A dominant follicle or corpus luteum could have a similar effect on the corresponding ovary. Accordingly, patients should be scanned during the early follicular phase to guard against this artefact in patients with regular menstrual function. Otherwise, patients with oligomenorrhoea might need to be rescanned if the initial examination showed a dominant follicle or corpus luteum. However, the presence of polycystic changes in the non active ovary would be adequate to make the diagnosis.
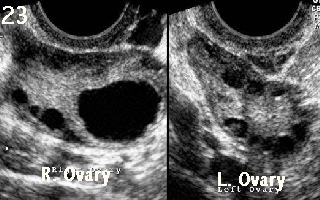
Images 21 and 22 show the same ovaries before and 8 months after using a combined oral contraceptive pill respectively. Note the loss of PCO pattern in figure 22. Image 23 show tow polycystic ovaries. The mature follicle in the right ovary did not conceal the PCO pattern on that side in this case.
The Syndrome
PCOS is
characterised by ovarian dysfunction with the important features of
hyperandrogenism, anovulation and polycystic ovaries on pelvic ultrasound scan
examination. It appears to have a familial tendency as 40 % of sisters
and 35% of mothers of affected women also have the syndrome (Kahsar-Miller et al 2001 (29). It should
be seen as a life long general medical condition rather than just a
fertility issue.
It usually has prepubertal onset especially
in girls with premature pubarche before the age of 8 years. It could be
triggered or unmasked by obesity, insulin resistance, and stress, or
dopaminergic dysregulation. A hypothalamic dysfunction has been suggested, as
pubertal women with PCOS had their LH surge at midday, rather than at midnight.
On the other hand, a dysfunctional pituitary gland has also been suggested,
because of the increased LH response to GnRH stimulation (Barnes et al 1989 (30). Furthermore, an ovarian role
has also been suggested related to abnormal activity of 17a-hydroxylase and 17/20 lyase (Rosenfield et al 1990 (31).
Over the years the emphasis on the study of
polycystic ovaries changed from a histological, to pure endocrine, then genetic
and ultrasound oriented, and lately metabolic. This is a good indication that
the exact cause or causes behind the development of PCOS are not yet well known.
It also proved that the condition is a heterogeneous one with different causes
in different patients. Nevertheless, once PCOS develops, the ovaries assume a
prime role in producing androgens (Goldzieher JW 1962, (32),
and Fisher et al 1974 (33).
Logically one could think of polycystic ovaries in 2 different ways; as normal
ovaries with abnormal gonadotrophins drive, or abnormal ovaries showing
abnormal morphology and response, irrespective of the gonadotrophins drive.
The essential anatomical features described
for PCO were reported as:
- Arrest
of follicular growth
- More
atretic cysts
- Relative
deficiency of healthy granulosa cells
- Predominance
of theca cells
- Increased
fibroblasts deposition in the follicles basal lamina due to increased
intraovarian androgens levels. This was thought to reduce the passage of FSH
into the follicles and reduce aromatase activation.
The biochemical changes related to PCO were
reported as:
- Theca
cells are hypersensitive to LH with increased production of androstenedione
compared to normal cases. Increased ovarian cytochrome P450c 17a activity is a
characteristic of polycystic ovaries. As it has 17a hydroxylase and
17, 20 lyase activities. It would promote more conversion of progesterone
to 17a-hydroxyprogesterone,
which is a substrate for androgens. Such increased activity was shown
after GnRH stimulation by Barnes et al in 1989 (30).
- Increased
production of inhibin B by the granulosa cells in response to androgens,
with the highest response following dihydrotestosterone exposure. This
would selectively affect FSH production.
- Exaggerated
LH response by the pituitary gland to GnRH stimulation in patients with
PCOS due to reduced dopamine effect. Infusion of dopamine in PCOS patients
with normal prolactin level reduces LH pulses 10 times more than in normal
women.
- There
is also dissociation of central opioids neurological activity in patients
with PCOS as shown by the lack of any effect of β-endorphins, which
normally inhibit LH release in normal women.
- Hyperinsulinaemia
due to abnormal peripheral resistance, as well as abnormal pancreatic beta
cell function has also been described. It has been suggested that insulin
resistance might be caused by excessive serine phosphorylation in the
insulin receptor, in at least 50% of patients with PCOS (Dunaif et Al 1985 (34).
Another explanation involved decreased action of chiroinsitol which is
necessary for induction of insulin signalling (Nestler
et al 1999 (35).
Different
reports described increased and normal levels of leptin in patients with PCOS. For
a given BMI, leptin was not different in PCOS vs. normal control (Caro F 1997 (36). A direct correlation of leptin to insulin has also
been reported and hyperleptinaemia has bee suggested to be part of the insulin
resistance syndrome (de Courten et al 1997 37). A
direct effect of leptin on liver function has been suggested as a cause for
insulin resistance. This is affected
through attenuation of tyrosine phosphorylation of
the insulin receptor substrate-1 (IRS-1) which is a major effect of
insulin, and down-regulation of gluconeogenesis. In contrast, leptin
increased the activity of IRS-1-associated phosphatidylinositol
3-kinase (Cohen et al 1996 38). Persistent activation of this
enzyme causes insulin resistance due to accelerated insulin-induced insulin receptor
substrate-1 degradation in adipocytes (Egawa et al 39).
Furthermore subcutaneous fat has been shown to be more effective than
intra-abdominal fat in causing high leptin levels (Vaulhonen et al 1998b 40). The variable results
regarding the level of leptin in patients with PCOS could be understood as the
insulin related leptin secretion is limited to insulin resistance in adipocytes
in women with PCOS (Jacobs and Conway 1999 41) Another
adipocytokine produced solely by adipose cells is adiponectin which is a 244
amino acid protein. It is thought to have a protective role against insulin
resistance (Weyer C et al 2001 42). Its level
has been reported to be low in women with PCOS, not related to obesity or
hyperinsulinaemia (Carmina et al 2005, 43).
The role of insulin in ovarian function is
essential, but has to be a balanced one. It is necessary for normal follicular
growth and maturation, as well as oestradiol production by the granulosa cells.
This phenomenon would be defective in cases of insulin deficiency. On the other
hand, excessive insulin exposure could enhance the androgenic pathway of the
theca cells to produce more androstenedione, creating a hyperandrogenic
intraovarian environment which could lead to anovulation and PCO formation.
Clinical presentation of women with PCOS
Women with PCOS might present with different
problems at different age groups, and treatment usually is tailored differently
to suit those different needs. This could be a reflection of the changes in the
range and severity of the symptoms themselves over the years, or the emphasis on
fertility needs by older women with irregular ovulation. In general terms, PCOS
is associated with hyperandrogenic symptoms and signs, obesity, irregular
periods and infertility. Some patients might have all the listed problems, but
show concern to one or two of them without any concern about the other signs.
This is especially so in teenage girls who are more concerned about their
weight and skin problems than irregular periods. Older women might be more
concerned about fertility issues, with minor if any concerns about excessive
hair growth or acne. They often choose to have induction of ovulation to help
them get pregnant rather than antiandrogens to help with their skin problems. Obesity
could be a real issue in the older age group, yet they might try to neglect its
implications, and seek advice to conceive nevertheless. This pattern is not rigid,
and patients in different age groups might present with the same concerns
Androgenic skin problems
Though young women might have problems with
acne, excessive weight gain and irregular periods, the first two problems rank
higher in their own minds. The disfiguring facial spots could affect their
lives, relationship with parents and peers and might lead to some psychological
problems. Hirsutism is also frequently seen in both young and older women.
It entails growth of dark terminal hair in a male distribution pattern, which
is not socially acceptable. Different ethnic groups have different numbers of
hair follicles per unit area of skin. Oriental women tend to have the least
number, compared to other races. Furthermore, the perception of how much hair
is unacceptable is different among different groups. However, a score
of more than 8 in the Ferriman-Gallwey scoring system
(44) is considered abnormal. Hirsutism is
generally related to exposure of the hair follicles to excessive androgens,
resulting in prolongation of the growth phase of the facial and body hair
cycle. An opposite effect might be seen on scalp hair follicles, with
androgenic alopecia being more common than the more severe frontal hair
recession, which is one of the signs of virilization. Hirsutism must be
differentiated from hypertrichosis which indicates excessive growth of ambosexual
hair which is seen in both women and men, mainly in the arms and legs. This is
more common as a familiar or genetic trait, but could be seen in patients on
glucocorticoid therapy.
Other androgenic skin problems
including greasy skin, androgenic alopecia and dandruff could also be seen.
Pigmentation of the skin could be seen mainly in association with insulin
resistance. Such problems include velvety dark patches called acanthosis
nigricans behind the neck, in the axillae and under the breasts. Skin tags or
flaps medically known as acrochordons or cutaneous papillomas could also be
present. Other names used included cutaneous tags, fibroma molluscum and
fibroepithelial polyps.
Obesity
Recording the body mass index (BMI) is
important in all patients presenting with anovulation or hyperandrogenic signs.
It is a good reflector of the amount of body fat, but not a perfect one. Nevertheless,
it is a good parameter to use in a clinical setup. All the same, its
significance should be related to the fat distribution areas, and the presence
of other cardiovascular diseases risk factors. The normal range is between 18.5
24.9 kg/m2, overweight range is 25-29.9 kg/m2, obesity
30-34.9 kg/m2, and severe obesity >35.0 kg/m2. Patients
with PCOS are at risk of developing obesity and figures between 40-50% have been
quoted (Goldzieher and Green 1963, 45, Lobo and Carmina
2000 46). It might even be a triggering factor during early puberty for
the development of the syndrome itself. It is usually of the android type,
which is a male characteristic with increased abdominal fat deposition. A waist
: hip ratio >0.85 in women indicates increased risk of cardiovascular diseases.
Alternatively, and more simply, the waistline could be used instead. A figure
>88 cm (35 inches) would be consistent with abdominal obesity in women.
Women with PCOS are prone to metabolic
problems related to obesity, high blood pressure, insulin resistance, high
insulin level, type II diabetes, high LDL cholesterol and triglycerides levels,
low HDL cholesterol, low fibrinolysis and alteration in plasminogen activator
inhibitor 1 (PAI-1). All these factors are related to Syndrome-X which is known
to increase the risks of cardiovascular accidents. However, many
epidemiological studies did not show increased risk of cardiovascular fatality
in women with PCOS (Pierpoint 1998 (47) and Wild et al
2000 (48)). This has been attributed to the high oestrogen environment
with its vasodilatory effects and high levels of vascular endothelial growth
factor in women with PCOS. Oestrogen acts on blood vessels wall eliciting
release of nitric oxide which is a potent vasodilator and improves blood flow (Gisclard et al 1988 49). Furthermore, women with
PCOS are 30 times more likely to experience obstructive sleep apnoea syndrome
(OSAS), in comparison to matched controls (Vgontzas
et al 2001 (50). Insulin resistance was a stronger risk factor of
the condition than BMI or testosterone level. Women with OSAS are also more
liable to snoring, interrupted night sleep, excessive daytime sleepiness and
easy fatigability The last authors also suggested that progressive
deterioration of PCOS leads to OSAS. High incidence of cholithiasis has also
been found in women with PCOS, even at a young age.
Beside it effect on insulin level, obesity
could aggravate the endocrine abnormalities in patients with PCOS through the
following means:
- High
levels of endorphins and dopamines in circulation
- High
hypothalamic opiates could alter GnRH pulse generation
- Tendency
to high prolactin levels
- High
conversion rate of androstenedione to oestrone creating a hyperoestrogenic
status
- Reduction
of SHBG production by the liver could lead to high free testosterone.
It is important to remember that not all
obese women with high insulin blood levels are hyperandrogenic. This could
emphasise the importance of local ovarian abnormalities which could make them
more liable to produce excessive amounts of androgens in response to
hyperinsulinaemia.
Problems with ovulation
The reproductive side in women with PCOS
could also be compromised with increased risk of anovulation,
menstrual abnormalities, ovarian hyperstimulation syndrome and cancer of the
endometrium. Ovulatory problems could show as inadequate or short luteal phase,
menorrhagia, polymenorrhoea, dysfunctional uterine bleeding, oligomenorrhoea
and amenorrhoea. However, it is more often for these patients to present with
oligomenorrhoea and dysfunctional uterine bleeding than any of the other mentioned
problems (Abdel-Gadir et al (3). The major impact
of PCOS on ovulation is affected through increased ovarian hyperandrogenic milieu,
as well as the effect of increased circulating androgens on the
hypothalamo-pituitary unit. Androgens are known to have a direct detrimental
effect on ovulation at the level of the ovaries as they could:
- Reduce
granulosa cells mitotic activity
- Reduce
FSH receptors on the granulosa cells
- Reduce
the FSH induced aromatase activity in the granulosa cells
- Reduce
LH receptors leading to reduced production of progesterone during luteal
phase, which could lead to abnormal uterine bleeding and menorrhagia.
- Reduce
oocytes maturation capacity
- Compromise
normal endometrial development and function.
- Reduce
pregnancy rate
All these problems could lead to disturbed
menstrual function and reduced fertility potential. The reproductive capacity of
patients with PCOS is also compromised by a higher risk of
hyperstimulation and multiple pregnancies, after induction of ovulation.
Furthermore, increased miscarriages rate has been documented by many authors in
relation to obesity or high LH, androgens, PAI-1, insulin resistance and
hyperinsulinaemia. Lower levels of glycodelin and insulin like growth factor binding
protein 1 (IGFBP-1), have been reported in patients with PCOS during the first
trimester of pregnancy (Jakubowicz et al 2004 51)
and in the non-pregnant state (Suikkari et al, 1989 52).
These two proteins are necessary for proper implantation by inhibiting the
immune response of the endometrium to the embryos. However, no association has
been firmly documented between PCOS and recurrent miscarriages, despite the
over representation of the presence of PCO in these cases (Essah PA et al 2004 53).
The same last authors related all the risk factors mentioned above to insulin
resistance and hyperinsulinaemia. Reducing the insulin blood level resulted in
reduction of LH, androgens and PAI-1, and increase in the level of glycodelin
and IGFBP-1 blood levels. In addition, patients with PCOS were shown to be at greater
risk of gestation diabetes and high blood pressure during pregnancy
irrespective of being insulin resistant or not. However, the risk of pre
eclampsia was high only in patient who were insulin resistant before getting
pregnant. Newborns from PCOS pregnancies were significantly more often delivered
by caesarean section and transferred to neonatal intensive care unit more often
than controls (Bjercke S et al, 2002 54).
Many studies documented reduced miscarriage rate with metformin (Khatab el al, 2006 55)
As many as 21% hyperandrogenic women with PCO
and regular menstruation were found to have anovulatory cycles (Carmina and Lobo 7). Similarly asymptomatic women with
ultrasonically diagnosed PCO and regular cycles had low luteal serum
progesterone level (Abdel-Gadir 3). This later
group might be the first stage in a continuous chain of events, passing through
a phase of regular anovulatory cycles, before they develop irregular and
anovulatory menstruation. This puts further emphasis on the point that the
presence of PCO even in women with regular menstrual cycles should not be considered
as a normal finding, and these patients might benefit of having regular follow
up.
Psychological effects of
PCOS
Women with PCOS are at risk of mood swings, anxiety and depression with
impaired quality of life (Benson S et al 2009 (56).
Obesity, hirsutism, irregular periods and subfertility were major sources of
psychological morbidity. However obesity was reported in one study to be the
most prevalent cause of mental distress, where as the impact of the other
symptoms proved to be less well defined (Bishop et al 2009
(57) and Adali et al 2008 (58)). A positive correlation has been
reported between the degree of insulin resistance, even before the outbreak of
type 2 diabetes, and the severity of depression (Timonen
et al, 2005 59). Such psychological difficulties might represent
disturbed stress responses by patients with PCOS, as shown by enhanced
hypothalamo-pituitary-adrenal axis and heart rate reactivity, as well as
reduced upregulation of IL-6 in response to stress (Benson
et al 2009, 60). This could be reflected biochemically with increased
catecholamines response to provoked stress. To improve the compromised quality
of life of this subgroup of patients, more attention should be paid to the
psychological impact of the disorder
Management
of patients with PCOS
Management of patients with PCOS is usually directed towards their mode
of presentation. However, the psychological impact of the problem should be assessed,
especially in the younger age group. The reason why they are seeking advice
should be ascertained, and dealt with though it might not be the more important
medical problem. Related medical problems could be controlled but might not be totally
cured. Furthermore, therapies would change with the age and needs of the patient.
Accordingly, prolonged follow up is necessary to prevent long term medical
problems. The management strategy should focus on:
- Reduction of body weight and
control of the metabolic dysfunction
- Treatment of peripheral
hyperandrogenisation
- Control of abnormal uterine
bleeding
- Treatment of infertility
It is not unusual for many patients to present with two or even all 4
problems together. Weight reduction is beneficial to all other 3 problems, and induction
of ovulation would help with anovulatory abnormal uterine bleeding as well, for
patients who are keen to get pregnant. However, treatment of skin
hyperandrogenic signs usually clashes with the treatment of infertility, as it
usually entails the use of drugs which block ovulation, or are contraindicated during
pregnancy.
Loss of
Weight
Excessive weight problems should be addressed as a priority, through
significant changes in life style, including more physical activity and healthy
eating. Self starvation should be avoided, as most women who lose weight
through starvation will regain their initial weight within 2-3
years. Adequate weight loss could lead to significant improvement in
insulin resistance, and reduces the level of circulating free androgens. It
could also help in regulating ovulation, and improves the chances of getting
pregnant. This could be done with a help of a dietician, and regular follow up
over a long period of time to guarantee compliance.
Unfortunately, most women would find it difficult to lose weight,
despite their serious attempts to do so. This might reflect the anabolic effects
of the high insulin and androgens levels. This is affected through improved
appetite at the level of the hypothalamus, reduced lipolysis and increased
lipogenesis. Accordingly, sustained self motivation, and professional help would
be needed. Metformin could be prescribed to patients with insulin resistance.
It would help with insulin utilisation at tissues level, especially the liver
and muscles. It could also reduce gluconeogenesis and glucose absorption from
the gastrointestinal tract. It usually causes gastrointestinal side effects,
and is better taken with food. The dose should be built up slowly to avoid side
effects and to allow compliance. The usual dose is 500 mg twice daily, but 850
mg tablets could be taken with food 3 times every day by non-responsive
patients. Metformin should be suspended few days before any major surgical
procedure. Reports of liver damage have been published (Chaudhry and Simmons 2001 (61), Nammour et
al 2003 (62), Kutoh
E, 2005 (63)), and severe elevation of hepatic
enzymes would give a good indication. Ideally, all patients should be tested
few times during the first year of medication and annually thereafter. Rarely,
it could be complicated with lactic acidosis.
Metformin use is contraindicated in patients with compromised hepatic or
renal function tests. Other contraindications include severe infections,
dehydration, alcoholism, heart failure, recent myocardial infarction and use of
X-ray contrast media. An important side effect of metformin is the
reduction of vitamin B12 absorption especially in patients who are at risk,
mainly vegetarians. However, it does not cause hypoglycaemia, but could dos so
if taken with alcohol. Nevertheless, it could normalise blood glucose level. To
have a good impact on insulin resistance and obesity, change in life style and
good feeding habits, as well as ample physical exercising are necessary. Metformin
is not a slimming drug.
Treatment
of skin hyperandrogenic signs
The 4 main strategies used in the treatment of female skin hyperandrogenisation
are:
- To assess the psychological
impact of the problem especially in young patients and offer the necessary
support when needed.
- To reduce adrenal and
ovarian androgens producton.
- To increase the level of
SHBG, which would reduce the free fraction of androgens.
- To use antiandrogens which
could block 5a-reductase activity at the
pilosebaceous organs, to reduce the conversion of testosterone to 5-dihydrotestosterone,
and by competing with the later at the skin receptors level.
- To use cosmetic means both
personally and through professional help.
Any androgenic medication should be changed or suspended. Predisposing
medical problems including adrenal hyperplasia, hyperprolactinaemia, or thyroid
dysfunction should be addressed first. Ovarian androgens production could be
reduced by blocking ovulation with an oral contraceptive pill. In certain
circumstances a glucocorticoid might be necessary, especially when an adrenal
enzymatic deficiency has also been diagnosed. The oestrogen fraction in any
combined oral contraceptive pill would also stimulate the liver to produce more
SHBG, to reduce the free fraction of androgens. However, the magnitude of this
increase in patients using ethinyl oestradiol in a daily dose of 30 µg was
found to be equivalent to SHBG level in women with regular menstrual cycles. A significant
increase was reported after using 50 µg daily, which is a high dose, not usually
used in most present day oral contraceptive pills. Currently, it is also believed
that pills with androgenic progestogens should be avoided, especially so, as they
could induce or worsen insulin resistance and might induce dislipidaemia. This
is especially so, as many pills devoid of such androgenic progestogens are now
available. Non androgenic progestogens include desogestrel, gestodene and
norgestimate. Examples of PCOS friendly pills include mercilon, yasmin, cilest,
marvelon, femodene, femodette and minulet. Metformin has also been shown to
reduce androgens production by acting directly on the ovaries, and could help
with skin problems even in patients who are not insulin resistant.
The most widely used antiandrogen nowadays is spironolactone which is an
aldosterone antagonist. Though initially used as a diuretic, it proved to have
excellent anti androgenic characteristics, with minimal side effects. It could take
few months before seeing a significant effect, and it usually sustains its
effect through the following mechanisms:
- It reduces testosterone
production by interfering with cytochrome P450 activity.
- It promotes the conversion
of testosterone to oestradiol in the liver.
- It reduces the activity of
the enzyme 5a-reductase necessary for the
conversion of testosterone to 5-dihydrotestosterone.
- It competes with 5-dihydrotestosterone
at the skin receptors.
The main side effect of spironolactone is intermenstrual bleeding which
usually settles with continued use. This is not a problem for patients using an
oral contraceptive pill which would also improve the clinical response by
inhibiting excessive ovarian androgens production. Using spironolactone during
the early weeks of pregnancy could lead to feminization of male fetus
genitalia. This follows its effect in reducing the concentration and activity
of 5-dihydrotestosterone, which is necessary for the development of male
external genitals. This is the idea behind the advice for using an oral
contraceptive pill, or any other effective method of contraception, by sexually
active women during their reproductive years, while on spironolactone. Changes
in blood electrolytes are not common but should be kept in mind, as
spironolactone is an anti aldosterone.
Other antiandrogens include cyproterone acetate, flutamide, finasteride
and dutasteride. The most widely used one in this group is cyproterone acetate,
either in a reversed sequential therapy as mentioned in chapter 4, or as part
of an oral contraceptive pill as in dianette (Schering UK). It has a potent
antigonadotrophic effect, and hence reduces ovarian androgens production. It
also has a direct effect at the skin level by competing with 5-dihydrotestosterone
for the receptor sites. It is important to combine it with an oestrogen, and
should be used only during the first half of the treatment course. This is
because of its long debo effect, which could cause menstrual dysfunction and
excessive uterine bleeding. It is recommended that cyproterone acetate should
not be used for a very long period of time after the symptoms have subsided.
This is even true for dianette, despite the small dose of cyproterone acetate,
as it has been shown to cause depression after prolonged use. Accordingly, dianette
should not be used for contraception purposes only, by non hyperandrogenic
women. Spironolactone in a daily dose of 100 mg has been shown to be more
effective on the skin than dianette which contains 3 mg cyproterone and 35 µg
ethinyl oestradiol. Other drugs are also potent but have significant hepatic
toxicity and should be used only sparingly, and only when really necessary. Flutamide
is an androgen receptor blocker given in a dose of 250 mg once or twice daily.
It has hepatic toxicity, and could alter liver function tests. It could also
cause anorexia, pruritis, dry skin and dark urine. It is mainly used for
resistant cases of androgenic alopecia. Liver function tests should be
performed before and regularly during the treatment. 5a-reductase inhibitors are not
very popular in treating female hyperandrogenisation, and could be less
effective than other antiandrogens. Finasteride (proscar) in a dose of 5 mg
every day could be used for the treatment of hirsutism as it is mainly a type 2
isoeznyme inhibitor. On the other hand, dutasteride (avodart) in a dose of 0.5
mg every day could inhibit both type 1 and 2 isoenzymes and causes a dramatic
reduction in dihydrotestosterone level within a short period of time. It has
been portrayed as an effective treatment for androgenic alopecia.
Using any of these medications should be combined with wise use of good
skin care and professional help for hair removal. Skin irritants should be
avoided. It is always advisable that patients should take a polaroid (or
digital) photograph before starting treatment, and at regular intervals
thereafter, for comparison purposes, and to monitor response. Laser treatment
proved to be effective in dealing with excessive hair growth, but should be
part of a general management plan, involving medical treatment of the excessive
androgens production.
A diagnosis of PCOS should also be considered
in hyperandrogenic women with polycystic ovaries despite having regular
menstruation. However, other causes of hyperandrogenism should be excluded
first. Furthermore, a high level of LH is no longer considered necessary to
confirm the diagnosis. It could be elevated in up to 60% of the patients, but
its level could be affected by recent ovulation, ingestion of certain
medications and BMI; being higher in leaner patients. Furthermore, it is
secreted in 90- minute pulses and the level could depend on the timing of
the sample within a pulse. In addition, the unreliability of single blood
sample hormone estimations in representing the true endocrine milieu has been
known since 1973 (Santen and Bardin 1973 64).
The reliability of a single LH estimation was undermined by a variability of
38% and 92% in accuracy to represent the 6-hour mean value, following 20
minutes blood sampling during the follicular and luteal phases of the cycle
respectively. The same authors suggested a minimum of 3-hour multiple sampling
to detect changes of 40% or less in LH concentrations. Such variability has
since been confirmed for LH as well as testosterone by Abdel
Gadir et al in 1991 (25). In this
respect, a high LH level is significant, but a normal level would not exclude
LH hypersecretion. This is a reflection of a stronger positive predictive
value, but a low negative one. However, the significance of measuring blood
levels of LH in anovulatory hyperandrogenic women with PCOS lies in its prognostic
value for selecting patients for ovarian electrocautery, as patients with high
LH levels had a better response (Abdel Gadir 65).
Idiopathic hirsutism
This is a term used to describe excessive hair growth not accounted for
by demonstrable excessive circulating androgens level. However, many of these
patients might have a subtle adrenal enzymatic deficiency. In many patients
only the free fraction of androgens is increased despite having normal total testosterone
and androstenedione levels. This could follow low levels of the carrier
molecule SHBG. Hepatic production of SHBG could be reduced by obesity, high
blood insulin and androgens as well as low thyroid hormone levels.
Increased end tissue (skin) sensitivity has been described as the
cause of excessive hair growth in cases of idiopathic hirsutism. This was
related to rapid turnover of androgens at the skin level, due to increased
numbers of androgen receptors, or increased conversion rate of testosterone to
the more biologically active dihydrotestosterone. This is related to an
increased 5a-reductase enzymatic activity, which is reflected by increased blood
levels of dihydrotestosterone metabolite 3a-androstandiol glucoronide (3a-diol G). Oral contraceptives do
not usually affect this end byproduct, which is usually reduced by
spironolactone and cyproterone acetate, which act as antiandrogens at the skin
level. This increased tissues turnover of androgens could explain why women
with the same circulating levels of androgens could have different degrees of
excessive hair growth. In this context, hirsutism is not a reflection of the
circulating level of androgens, but rather an expression of the skin turnover
of 5-dihydrotestosterone, as reflected by the increased level of 3a-diol glucuronide. However, this
metabolite byproduct is produced by many tissues in the body, which dampened
the initial enthusiasm for using it as a sole marker of idiopathic hirsutism.
Infertility
treatment of patients with PCOS
Infertile obese women with PCOS should be offered fertility
treatment only after a good effort has been invested in losing
weight. This has been shown to improve ovulation and increase their
chances of natural conception, even without any medication. The risk of
increased miscarriage in obese women with PCOS after induction of ovulation
should be kept in mind (Bohrer and Kemmann 1987
(66), Abdel-Gadir et al 1990, (26). This is on
top of the real risk of gestational diabetes and associated fetal and maternal
complications.
Induction of ovulation should be attempted
first with clomiphene citrate under supervision because of the risk of multiple
ovulations. A starting dose of 50 mg every day for 5 days could be started on
the 3rd day of withdrawal bleeding. Ovulation usually occurs about
5-7 days after the last tablet. A higher dose of 100 mg every day for 5 days
might be needed. Higher doses would usually be ineffective and could affect the
cervical mucus fluidity, increase the histological aging of the endometrium
relative to the follicle, and interfere with tubal motility and fluid chemistry
as an antioestrogen. Treatment with clomiphene should not be continued for more than 6 cycles. Gonadotrophins
could be used in nonresponsive cases, but they need special expertise, and easy
access to professional ultrasound monitoring. Attempts should be made to aim at
monofollicular ovulation by starting medication with a single ampoule for 7-10
days, before increasing the dose in half an ampoule doses, at equal time
spacing. The cycle should be abandoned if multiple follicles were recruited.
The risk of multiple follicular development could exceed 50% and 80% with clomiphene
citrate and gonadotrophins therapy respectively in patients with PCOS. Ovarian
diathermy has been advocated as an alternative to gonadotrophins, with good
outcome. In fact 52.1-84% of patient with the sole problem of PCOS conceived
after such a procedure (Abdel-Gadir et al 1990 (26),
Gjönnaess H, 1994 (67)), which proved to be as
effective as gonadotrophins in inducing ovulation and pregnancy rate, with no
risk of hyperstimulation or multiple pregnancies (Abdel-Gadir
1990 - 26). A lower risk of miscarriages has also been reported after
ovarian electrocautery (Abdel-Gadir - 26). The same last authors reported better endocrine response
in patients with PCOS and high LH level compared to those with normal LH level
but high LH:FSH ratio (Abdel Gadir 65). A further benefit of laparoscopy
in these cases is that it offers a good chance to examine the pelvis for other
infertility factors at the same time. The risk of developing pelvic adhesions
after ovarian drilling should be weighed against the prospective benefits
expected in these patients. Such risk
could be reduced by adopting principles used during microsurgery (Abdel Gadir 1993 68):
- Insert the needle at right
angle to the surface of the ovary to prevent slit cauterisation and reduce
the damaged ovarian surface area.
- Apply the current only when
the needle touches the ovary to prevent arcing and charring of the ovarian
surface which could lead to adhesions formation.
- Use the minimum number of
points according to the ovarian size
- Cool the ovary with a physiological
solution as soon as that side is done
- Avoid electrocautery in
women with evidence of PID or had extensive pelvic surgery with large raw
areas especially on the pelvic sidewall, as this would encourage ovarian
adhesions to these areas.
Metformin has been shown to be highly effective in augmenting clomiphene
citrate activity for induction of ovulation in previously resistant patients (Siebert TI et al 2006, 69). This could lead
to reduction in androgen production by the ovaries, better ovulation and
reduced miscarriage rates. Reduction of insulin level has been shown to reduce
ovarian cytochrome P450c17a activity and serum free testosterone (Nestler et al 1996, 70). Furthermore, it has been
shown to reverse the metabolic and endocrine risk factors associated with
increased miscarriage rate in women with PCOS. Other than reducing the level of
androgens, it also reduces the levels of PAI-1, and luteinising hormone.
However, it might take 4 months before a full molecular effect is
achieved. Recent reports suggested that it might have a direct effect on
the ovaries, even in women who are not insulin resistant (Tan S et al, 71).
Implications of ultrasonically diagnosed PCO in
non-PCOS patients
Normal women with
polycystic-appearing ovaries
It has been reported that 16-25% of 'normal'
women had polycystic-appearing ovaries without any specific symptoms or signs (Polson 2, Abdel-Gadir 3,
and Wong 4). However, many of them might have
increased risks and similar morbidity as related
to PCOS. They have been reported to show subtle metabolic (Carmina et al 72) and endocrine (Abdel-Gadir et al 1992 3, and Chang et al 8) abnormalities
including:
- Low high density lipoprotein-cholesterol
- Evidence of insulin resistance
- Androgenic ovarian response to
stimulation with gonadotrophins
- Low serum progesterone during the luteal
phase of natural cycles indicating ovulatory dysfunction.
Furthermore, they have the same risk of
excessive response to induction of ovulation and ovarian hyperstimulation syndrome
as patients with PCOS. In addition, Doppler studies showed normal women with
PCO had similar uterine and ovarian blood flow as patients with PCOS (Zaidi et al 73). Accordingly, the notion that the
presence of PCO in this group of women is totally normal should be revised.
Other endocrine problems
associated with ultrasonically diagnosed PCOS
Polycystic ovaries could be seen in women
with a wide range of different endocrine problems including:
- Hypothyroidism
- High
prolactin level
- Adrenal
enzymes deficiencies
- Hypothalamic
dysfunction
Accordingly, total reliance on
ultrasonography alone would create a diagnostic problem, and wise utilisation
of endocrine investigations would be necessary (Abdel-Gadir
et al 1992 3).
Hypothyroidism
As many as 36.4% patients
with hypothyroidism have shown PCO on ultrasound scan examinations (Abdel-Gadir 3). This could be a good representation of
normal ovaries which changed polycystic due to abnormal external impulses, as alluded
to before. Thyroxine is needed for the production of SHBG, and patients with
hypothyroidism have lower levels than normal. This would lead to increased
level of free androgens in circulation, which could be aromatised in the
hypothalamus leading to changes in the gonadotrophins pulse secretion, which
could affect the ovaries negatively. Secondly, high androgens could affect the
ovaries directly leading to reduction in FSH and LH receptors, reduced
aromatase activity, and development of PCO. Furthermore, the effect of
hypothyroidism could lead to TRH induced secondary hyperprolactinaemia in these
patients.
Hyperprolactinaemia
Polycystic ovaries
have been reported in 50.0 % of patients with hyperprolactinaemia (Abdel Gadir et al 1992 3). High prolactin could affect
the ovaries in the following ways:
- It could affect GnRH pulse generation and
accordingly pituitary gonadotrophins production
- It has a direct effect on the follicles at a
postreceptor level, reducing their response to gonadotrophins.
- It increases adrenal androgens production by
causing partial enzymatic block leading to a hyperandrogenic state.
Adrenal enzymatic deficiencies
Partial enzymatic deficiencies have been discussed thoroughly in chapter
4. They could be seen at puberty or early adult life, and are described to be
of adult onset. The most common variety is partial deficiency of the 21a-hydroxylase enzyme to different
extent in different patients. All adrenal enzymatic deficiencies are autosomal
recessive genetical problems, inherited from either or both parents. The
pattern of presentation could include symptoms and signs similar to those
described for PCOS. In fact the ovaries could be polycystic in virtually 100%
of the cases (Abdel-Gadir et al 1992 3). The
American College of Obstetrics and Gynaecology recommended that all women with
a suspected diagnosis of PCOS should be screened for 17a-hydroxyprogesterone levels.
Hypothalamic
dysfunction
Hypothalamic dysfunction is a diagnosis of omission, when all known
causes capable of causing ovulatory dysfunction have been excluded. Many non
measurable factors could be involved in these cases, such as severe stress
which is known to affect GnRH pulse generation. Also weight-related problems
could affect the ovaries, but they have been associated more with multicystic
rather than polycystic ovaries. Medication could have a similar effect,
especially so for antiepileptic drugs and all other drugs capable of affecting
the brain neurotransmitters, and accordingly GnRH pulse generation.
Despite the lack of an overt endocrine dysfunction that could be
revealed by a peripheral blood test, polycystic ovaries were reported in 23.7%
of anovulatory patients with hypothalamic dysfunction (Abdel
Gadir et al 1992 3). Such ovaries would behave the same way as any other
polycystic ones with increased risk of hyperstimulation during induction of
ovulation. Treatment of patients in this group should be tailored to their
needs and their symptoms. This could involve induction of ovulation to
facilitate conception. An oral contraceptive pill could be used to induce
regular withdrawal bleeding and protect against unwanted pregnancies. Regular
progestogen withdrawal bleeding every 8 weeks would guard again endometrial
hyperplasia in patients who are not sexually active.
Effect of
age on patients with PCOS
With advancing age, women with PCO tend to have more regular periods,
lower circulating androgens (Winters et al 2000, (74)), and loss of the PCO pattern (Abdel Gadir et al 2009, 23). These changes could be
secondary to the age related reduction in the total number of recruitable follicles
and the increase in FSH level leading to a more favourable LH / FSH
ratio. However, obese patients with PCOS are more likely to develop type II
diabetes. A figure of 80% risk of type II diabetes by the age 40 years has been
quoted in this subgroup. They are also at more at risk of carcinoma of the
endometrium, especially in the presence of other risk factors including
amenorrhoea, endometrial hyperplasia, and high blood pressure.
Summary
PCOS is a heterogeneous condition involving interlinked metabolic,
endocrine and reproductive problems. Its exact cause is not yet well known, but
many theories have been put forward to explain its development. It has a
familial predisposition, though an exact genetic or chromosomal cause has not
been established. More evidence is accumulating relating it to abnormal insulin
resistance and hyperinsulinaemia. It should be treated as a general medical
problem, rather than just a fertility issue. Controlling the metabolic disorder
by reducing body weight and reducing insulin resistance should be the primary
management objective. This would impact favourably on the endocrine and
reproductive sides of the syndrome. The presence of ultrasonically diagnosed
PCO in patients with menstrual irregularity and hyperprolactinaemia, or thyroid
and adrenal dysfunction, stresses the need for a proper endocrine assessment.
This would help in making a definitive diagnosis before starting any form of
medical or surgical treatment solely on the ultrasonic findings.
References
1. Knochenhauer E, Key TJ,
Kahsar-Miller M, Waggoner w, Boots LR and Azziz R. Prevalence of polycystic
ovary syndrome in unselected black and white women of southeastern United
States: a prospective study. J Clin Endocrinol Metab 1998; 83(9): 3078-3082.
2. Polson DW, Adam J, Wadsworth J
and Franks S. Polycystic ovaries a common finding in normal women. Lancet
1988; 1: 870-871.
3. Abdel Gadir, A., Khatim MS.
Mowafi RS, Alnaser HM, Muharib NS and Shaw RW. Implications of ultrasonically diagnosed polycystic
ovaries (1)-Correlation with basal hormonal profiles. Human Reproduction 1992;
7 (4), 453-457.
4. Wong LI, Morris
RS, Legro R, Paulson RJ and Sauer MV. Isolated polycystic morphology in ovum
donors predicts response to ovarian stimulation. Hum Rep 1995; 10: 524-528.
5. Shiono H. Dermatoglyphics in medicine. Am J Forensic Med
Pathol 1986; 7 (2): 120-6.
6. Katznelson M and Goldman B. Fetal dermatoglyphics. Clin
Genet 1982; 21 (4): 237-42.
7. Carmina E and Lobo RA. Do hyperandrogenic women with normal menses have
polycystic ovary syndrome? Fertil Steril 1999; 71: 319-322.
8. Chang PL, Lindheim SR, Lowre C et al. Normal ovulatory
women with polycystic ovaries have hyperandrogenic pituitary-ovarian response
to gonadotrophin-releasing hormone agonist testing. JCE & M 2000;
85(3):995-1000.
9. Farquhar C. History of polycystic ovary syndrome. In:
Polycystic Ovary
Syndrome. Edited by: Gabor T. Kovacs. Cambridge University Press 2000, Chapter
2, pp 4-22.
10.10. ODowd MJ, Philipp EE and Phillip
EE. Chromosomal,
hormonal and psychogenic amenorrhoea and oligomenorrhoea. In: History of
Obstetrics and Gynaecology. Informa Healthcare 2000, pp 307-316.
11.Stein IF and Leventhal ML. Amenorrhoea associated
with bilateral polycystic ovaries. Am J Obstet Gynecol 1935; 29: 181-186.
12.McArthur JW, Ingersoll FM and Worchester J. Urinary
excretion of interstitial-cell and
follicle stimulating hormone activity by women with diseases of the
reproductive system. J Clin Endocrinol Metab 1958; 18: 1202-1215.
13.De Vane GW, Czekala NM, Judd HL et al. Circulating
gonadotrophins, oestrogens and androgens in polycystic ovarian disease. Am J.
Obstet Gynecol 1975; 121: 496-500.
14.Rebar R, Judd HL and Yen SS, Rakoff J, Vandenberg G
and Naftolin F. Characterisation of the inappropriate gonadotropin secretion in
polycystic ovary syndrome. J Clin Invest 1976; 57(5): 1320-9.
15.Swanson M, Sauerbrei EE and Cooperberg PL. Medical
implications of ultrasonically detected polycystic ovaries. J Clin Ultras 1981;
9(5): 219-222.
16.Hann LE, Hall DA,
McArdle CR and Seibel M. Polycystic ovarian disease: sonographic spectrum.
Radiology 1984; 150(2): 531-534
17.Adam J, Franks S, Polson DW and Mason HD.
Multifollicular ovaries: clinical and endocrine features and response to
pulsatile gonadotropin releasing hormone. Lancet 1985; 2: 1375-9
18.Kahn CR, Flier J, Bar RS, Archer JA, Gorden P,
Martin MM and Roth J. They syndrome of insulin resistance and acanthosis
nigricans. Insulin receptor disorder in man. N Engl J Med 1976; 294(14):
739-745.
19.Revised 2003
consensus on diagnostic criteria and long-term health risks related to
polycystic ovary syndrome. Fertil Steril 2004; 81(1):19 25.
20.Hughesdon P. Morphology
of morphogenesis of the stein-leventhal ovary and so called hyperthecosis.
Obstet Gynecol Surv 1982; 37: 59-77.
21.Maciel GA, Baracat EC,
Benda JA, Markham SA, Hensinger K, Chang RJ and Erickson GF. Stockpiling of
transitional and classic primary follicles in ovaries of women with polycystic
ovary syndrome. J Clin Endocrinol Metab 2004; 89: 5321-5327.
22.Webber LJ, Stubbs S,
Stark J, Trew GH, Margara R, Hardy K and Frank S. Formation and early
development of follicles in the polycystic ovaries. Lancet 2003; 362:
1017-1021.
23.Jonard S and Dewailly D.
The follicular excess in polycystic ovaries, due to intraovarian
hyperandrogenism, may be the main culprit for the follicular arrest. Hum Reprod
Update 2004; 10(2): 107-110.
24.Abdel-Gadir A, Oyawoye O and Chander B. Coexistence of polycystic ovaries
and uterine fibroids and their combined effect on the uterine arteries blood
flow in relation to age and parity. The Journal of Reproductive Medicine 2009;
54: 347-352.
25.Yen SSC. Chronic anovulation caused by peripheral endocrine
disorders. In Reproductive Endocrinology, Physiology, Pathophysiology and
Clinical Management. Ed. Yen SSC and Jaffe MD, WB Saunders Company.
Philadelphia, pp 441-499.
26.Abdel Gadir A,
Khatim MS, Mowafi RS, Alnaser HM, Alzaid HGN and Shaw RW. Polycystic ovaries: Do these represent a specific
endocrinopathy? British Journal of Obstetrics and Gynaecology 1991, 98,
300-305.
27.Abdel Gadir A,
Mowafi RS, Alnaser HM, Alrashid AH, Alonezi OM and Shaw RW. Ovarian
electrocautery versus human menopausal gonadotrophins and pure follicle
stimulating hormone therapy in the treatment of patients with polycystic
ovarian disease. Clin Endocrinol 1990; 33: 585-592.
28.Givens RJ, Andersen RN,
Umstol ES and Wiser WL. Clinical findings and hormonal responses in patients
with polycystic ovarian disease with normal versus elevated LH levels. Obstet
Gynecol 1976; 47: 388-394.
29.Kahsar-Miller MD, Nixon
C, Boots LR, Gor RC and Aziz R. Prevalence of polycystic ovary syndrome (PCOS)
in first degree relatives of patients with PCOS. Fertil Steril 2001; 75: 53-58.
30.Barnes R, Rosenfield RL.
Burstein S and Ehrmann DA. Pituitary ovarian response to nafarelin testing in
the polycystic ovary syndrome. N Engl J Med 1989; 320(9): 559-65.
31.Rosenfield RL, Barnes
RB, Cara JF and Lucky AW. Dysregulation of cytochrome P450c 17 alpha as the
cause of polycystic ovarian syndrome. Fertil Steril 1990; 53(5): 785-791.
32.Goldzieher J and Green
J. The polycystic ovary: 1. Clinical and histological features. J Clin
Endocrinol Metab 1962; 22: 325-338.
33.Fisher ER, Gregorio r,
Stephen T, Nolan S and Donowski TS. Ovarian changes in women with morbid
obesity. Obstet Gynecol 1974; 44: 839-844.
34.Dunaif A, Xia j, Book
CB, Schenker E and Tang Z. Excessive insulin receptor phosphorylation in
cultured fibroblasts and in skeletal muscle. A potential mechanism for insulin
resistance in polycystic ovary syndrome; F Clin Invest 1985; 96: 801-810.
35.Nestler JE, Jakubowicz
DJ, Reamer P, Gunn RD and Allan G. Ovulatory and metabolic effects of a
D-chiro-inositol in the polycystic ovary syndrome. N Engl J Med 1999; 340:
1314-1320.
36.Caro J G. Editorial: Leptin is normal in PCOS, an editorial
about three negative papers. J Clin Endocrinol Metab 1997; 82(6): 1685-6.
37.de Courten M, Zimmet P, Hodge A, Collins V, Nicolson M,
Staten M, Dowes G and Alberti KG. Hyperleptinaemia: the missing link in the
metabolic syndrome? Diab Med 1997; 14(3): 200-208.
38.Cohen B, Novick D and Rubinstein
M. Modulation of insulin activity by leptin. Science 1996; 274.
(5290): 1185 1188.
39. Egawa K, Nakashima K,
Sharma PM, Maegawa H, Nagai Y, Kashiwagi A, Kikkawa R and Olefsky JM. Persistent
activation of phosphatidylinositol 3-Kinase causes insulin resistance due to
accelerated insulin-induced insulin receptor substrate-1 degradation in 3T3-L1
adipocytes. Endocrinology 2000; 141(6): 1930-1935.
40. Vauhkonen I, Niskanen L, Haffner S, Kainulainen S, Uusitupa
M and Laakso M. Insulin resistant is associated with high serum leptin levels
in offspring of patients with non-insulin-dependent diabetes mellitus. Eur J
Endocrinol 1998; 139(6): 598-604.
41.Jacobs HS and Conway GS. Leptin, polycystic ovaries and polycystic
ovary syndrome. Hum Reprod Update 1999; 5(2): 166-171.
42.Weyer C, Funahashi T, Tanaka S, Hotta K, Matsuzawa Y,
Pratley RE and Totaranni PA. Hyppoadiponectinemia in obesity and type 2
diabetes: close association with insulin resistance and hyperinsulinaemia. J
Clin Endocrinol Metab 2001; 86: 1930-1935.
43.Carmina E, Orio F, Palomba S, Cascella T, Longo RA, Colao
AM, Lombardi G and Lobo RA. Evidence for altered adipocyte function in
polycystic ovary syndrome. Eur J Endocrinol 2005; 152: 389 394.
44.Ferriman D and Gallwey JD. Clinical
assessment of body hair growth in women. J Clin Endocrinol 1961; 21: 1440-1447.
45.Goldzieher J and Green
J. Clinical and biochemical features of polycystic ovarian disease. Fertil
Steril 1963; 14: 631-653.
46.Lobo O and Carmina E.
The importance of diagnosing the polycystic ovary syndrome. Ann Intern Med
2000; 132(12): 989-993.
47.Pierpoint T, McKeigue
PM, Isaacs AJ, Wild SH and Jacobs HS. Mortality of women with polycystic ovary
syndrome at long-term follow-up. J Clin Epidemiol 1998; 51(7): 581-586.
48.Wild S, Pierpoint T,
McKeigue P and Jacobs H. Cardiovascular disease in women with polycystic ovary
syndrome at long-term follow-up: a retrospective cohort study. Clin Endocrinol
2000; 52(5): 595-600.
49.Gisclard V, Miller VM
and Vanhoutte PM. Effect of 17 beta oestradiol on endothelium-dependent
responses in the rabbit. J Pharmacol Exp Ther 1988; 244: 19-22.
50.Vgontzaz AN, Legro RS,
Bixler EO, Grayev A, Kales A and Chrousos GP. Polycystic
ovary syndrome is associated with obstructive sleep apnoea and daytime
sleepiness: Role of insulin resistance. J Clin Endocrinol Metab 2001; 86(2):
517-520.
51.Jakubowicz DJ, Essah PA, Seppäläl M, Jakubowicz S, Baillargeon JP, Koistinen R
and Nestler JE. Reduced serum glycodelin and insulin
like growth factor binding protein01 in women with polycystic ovary syndrome
during the first trimester of pregnancy. J Clin Endocrinol Metab 2004; 89:
833-839.
52.Suikkari AM, Ruutianinen K, Erkkola R, Seppala M. Low levels of low molecular weight insulin-like growth
factor-binding protein in patients with polycystic ovarian disease. Hum Reprod
1989; 4: 136-139.
53.Essah PA, Cheang KI and Nestler JE. The
pathophysiology of miscarriages in women with polycystic ovary syndrome. Review
and proposed hypothesis of mechanisms involved. Hormones 2004; 3(4): 221-227.
54.Bjercke S, Dale PO, Tanbo T, Storeng R,
Ertzeid G and Abyholm T. Impact of insulin resistance on pregnancy
complications and outcome in women with polycystic ovary syndrome. Gynecol
Obstet Invest 2002; 54(2): 94-98.
55.Khatab S, Mohsen IA, Foutouh IA, Ramadan
A, Moaz M and Al- Inany H. Metformin reduces abortion in pregnant women with
polycystic ovarian syndrome. Gynecol Endocrinol 2006; 22(12): 680-684
56.Benson S, Hahn S, Tan S, Mann K, Janssen
OE, Schedlowski M and Elsenbruch S. Prevalence and implications of anxiety in
polycystic ovary syndrome: results of an internet-based survey in Germany. Hum
Reprod 2009; 24(6): 1446-1451.
57.Bishop SC, Basch S and Futterweit W.
Polycystic ovary syndrome, associated depression and affective disorders. Endocr
Pract 2009; 6: 1-31.
58.Adali E, Yildizhan R, Kurdoglu M,
Kolusari A, Edirne T, Sahin HG, Yildizhan B and Kamaci M. They relationship
between clinico-biochmemical characteristics and psychiatric distress in young
women with polycystic ovary syndrome. J Int Med Res 2008; 36(6): 1188-1196.
59.Timonen M, Laakso M, Jokelainen J, Rajala
U, Meyer-Rochow VB and Keinänen-Kiukaanniemi S. Insulin resistance and
depression: cross sectional study. BMJ 2005; 330: 17-18.
60.Benson S, Arch PC, Tan S, Mann K, Rifaie
N, Janssen OE, Schedlowski M and Elsenbruch S. Disturbed stress response in
women with polycystic ovary syndrome. Psychoneuroendocrinology 2009, 34(5):
727-735.
61.Chaudhry MU and Simmons DL. Case of the
month, hepatic and renal failure in a patient taking troglitazone and
metformin. J Ark Med Soc 2001; 98(1): 16-19.
62.Nammour FE, Fayad NF and Peikin SR.
Metformin-induced cholestatic hepatitis; Endocr Pract 2003; 9(4): 3070309
63.Kutoh E. Possible metformin-induced
hepatotoxicity. Am J Geriatr Pharmacother 2005; 3(4): 270-273.
64.Santen RJ and Bardin CW. Episodic
luteinising hormone secretion in man. Pulse analysis, clinical interpretation,
physiologic mechanisms. J Clin Invest 1973; 52: 2617-2628.
65.Abdel Gadir A,
Khatim MS, Alnaser HM, Mowafi RS and Shaw RW. Ovarian electrocautery: Responders versus non-responders.
Gynaecological Endocrinology 1993; 7, 43-48.
66.Bohrer M and Kemmann E. Risk factors for spontaneous
abortion in menotropin-treated women. Fertil Steril 1987; 48: 571-575
67.Gjönnaess
H. Ovarian electrocautery in the treatment of women with polycystic ovary
syndrome (PCOS). Factors affecting results. Acta Obstet Gynecol Scand 1994;
73(5): 407-12.
68.Abdel
Gadir A. Ovarian surgery. In: The control and stimulation of follicular growth.
Advances in Reproductive Endocrinology. Volume 5, PP 111-124. Edit RW Shaw, The
Parthenon Publishing Group, Casterton Hall, Carnforth, Lancs. 1993.
69.Siebert TI, Kruger TF, Steyn DW and Nosarka S. Is addition of metformin efficacious in
the treatment of clomiphene citrate-resistant patients with polycystic ovary
syndrome? A structured literature review. Fertil Steril 2006; 86(5): 1432
1437.
70.Nestler JE and
Jakubowicz DJ. Decreases in ovarian cytochrome P450c17a activity and serum free testosterone after
reduction of insulin secretion in polycystic ovary syndrome. New Eng J Med
1996; 335(9): 617-623.
71.Tan S, Hahn S, Benson S, Dietz T, Lahner H, Moeller LC, Schmidt M,
Elsenbruch S, Kimmig R, Mann K and Janssen OE. Metformin improves polycystic ovary syndrome
symptoms irrespective of pre-treatment insulin
resistance. Eur J
Endocrinol 2007; 157:
669676.
72.Carmina E, Wong
L, Chang L, Paulson RJ, Sauer MV, Stanczyk FS and Lobo RA. Endocrine
abnormalities in ovulatory women with polycystic ovaries on ultrasound. Hum Rep
1997; 12(5): 905-909.
73.Zaidi J. Blood
flow changes in the ovarian and uterine arteries in women with normal and
polycystic ovaries. Hum Fertil (Camb) 2000; 3: 194-198.
74.Winters SJ, Talbott E, Guzick DS,
Zborowski J and McHugh KP. Serum testosterone levels decrease in middle age in
women with polycystic ovary syndrome. Fertil Steril 2000; 73: 724-729.
75.Takahashi K, Yoshino K, Nishigaki A, Eda Y and
Kitao M. On the relationship between endocrine and ovulatory abnormalities and
polycystic as diagnosed by ultrasonography. Int J Fertil 1992; 37(4): 222-6.
76.Gonzalez F, Chang L,
Horab T and Lobo RA. Evidence for heterogeneous etiologies of adrenal
dysfunction in polycystic ovary syndrome. Fertil Steril 1996; 6(3): 354-361.
77.Legro RS, Finegood D and
Dunaif A. A fasting glucose to insulin ratio is a useful measure of insulin
sensitivity in women with polycystic ovary syndrome. J Clin Endocrinol Metab
1998; 83(8): 2694-2698.
78.Chang RJ, Lindheim SR,
Lowre C, Ferin M, Gonzalez F, Berglund L, Carmina E, Sauer MV and Lobo RA.
Normal ovulatory women with polycystic ovaries have hyperandrogenic pituitary
ovarian responses to gonadotropin-releasing hormone agonist testing. J Clin
Endocrinol Metab 2000; 85(3): 995-1000.
79.Lobo RA and Carmina E.
The importance of diagnosing polycystic ovary syndrome. Annals of Int Med 2000;
132(12): 989-93.
80.Ehrmann DA, Sturis J,
Byrne MM, Karrison T, Rosenfield RL, Polonsky KS. Insulin secretory defects in
polycystic ovary syndrome. Relationship to insulin sensitivity and family
history of non-insulin-dependent diabetes mellitus. J Clin Invest 1995; 96:
520-527.